State Variation in Primary Care Physician Supply: Implications for Health Reform Medicaid Expansions
HSC Research Brief No. 19
March 2011
Peter J. Cunningham
Under the Patient Protection and Affordable Care Act (PPACA), Medicaid enrollment is expected to grow by 16 million people by 2019, an increase of more than 25 percent. Given the unwillingness of many primary care physicians (PCPs) to treat new Medicaid patients, policy makers and others are concerned about adequate primary care capacity to meet the increased demand. States with the smallest number of PCPs per capita overall—generally in the South and Mountain West—potentially will see the largest percentage increases in Medicaid enrollment, according to a new national study by the Center for Studying Health System Change (HSC). In contrast, states with the largest number of PCPs per capita—primarily in the Northeast—will see more modest increases in Medicaid enrollment. Moreover, geographic differences in PCP acceptance of new Medicaid patients reflect differences in overall PCP supply, not geographic differences in PCPs’ willingness to treat Medicaid patients.
The law also increases Medicaid reimbursement rates for certain services provided by primary care physicians to 100 percent of Medicare rates in 2013 and 2014. However, the reimbursement increases are likely to have the greatest impact in states that already have a large number of PCPs accepting Medicaid patients. In fact, the percent increase of PCPs accepting Medicaid patients in these states is likely to exceed the percent increase of new Medicaid enrollees. The reimbursement increases will have much less impact in states with a relatively small number of PCPs accepting Medicaid patients now because many of these states already reimburse primary care at rates close to or exceeding 100 percent of Medicare. As a result, growth in Medicaid enrollment in these states will greatly outpace growth in the number of primary care physicians willing to treat new Medicaid patients.
- Will Medicaid Coverage Ensure Access?
- How the Study Was Done
- Geographic Variation in PCP Supply
- Acceptance of New Medicaid Patients
- State Differences in Relative Supply of Medicaid PCPs
- Potential Effects of Health Reform
- Supply of Specialists
- Policy Implications
- Notes
- Data Source and Methods
- Supplementary Tables
Will Medicaid Coverage Ensure Access?
![]() nder federal health reform, Medicaid eligibility will expand to cover as many as 16 million more poor and low-income adults by 2019.1 Although the coverage expansion is expected to substantially increase access to medical care, many are concerned that the increased demand will exceed the capacity of local health care delivery systems, particularly the supply of primary care physicians. Thus, while health reform is likely to decrease financial barriers to care, other barriers—especially the availability of physicians and the ability to get timely appointments—could increase.
nder federal health reform, Medicaid eligibility will expand to cover as many as 16 million more poor and low-income adults by 2019.1 Although the coverage expansion is expected to substantially increase access to medical care, many are concerned that the increased demand will exceed the capacity of local health care delivery systems, particularly the supply of primary care physicians. Thus, while health reform is likely to decrease financial barriers to care, other barriers—especially the availability of physicians and the ability to get timely appointments—could increase.
Physician capacity is a special concern in Medicaid because fewer physicians accept Medicaid patients relative to Medicare and privately insured patients, primarily because of low reimbursement rates.2 To address this, PPACA, as amended by the Health Care and Education Reconciliation Act of 2010, increases Medicaid reimbursement rates for certain evaluation and management services provided by primary care physicians to 100 percent of Medicare rates in 2013 and 2014. The impact of the reimbursement increase likely will be limited because of its temporary nature and exclusion of other services provided by PCPs and any services provided by medical and surgical specialists.3 In addition, other factors contribute to physicians’ willingness to treat Medicaid patients, including delayed reimbursement, paperwork and high administrative burden, and low compliance among patients.4
Potential problems with Medicaid physician capacity likely will vary considerably across states because of differences in states’ overall physician supply and Medicaid reimbursement rates, which affect the number of physicians who accept Medicaid patients.5 In addition, states also differ in terms of the relative number of people currently enrolled in Medicaid, as well as the number of people who will gain Medicaid eligibility in 2014.6 Ideally, states with the greatest increase in Medicaid enrollment would be the same states that experience the greatest increase in PCP capacity when reimbursement rates for primary care rise. Conversely, PCP shortages in some states will get much worse if there are large increases in Medicaid enrollment that outpace any gains in Medicaid PCP capacity.
The objective of this study was to examine state variation in Medicaid PCP supply, taking into account:
- the overall supply of PCPs in the state;
- the proportion of PCPs who accept Medicaid patients; and
- the number of nonelderly Medicaid enrollees in the state.
The study also examines how state variation in Medicaid PCP supply is likely to change after the eligibility expansions take place in 2014. The analysis takes into account both the potential number of new Medicaid enrollees in a state, as well as the potential increase in the number of PCPs accepting Medicaid patients when reimbursement rates for primary care services increase to 100 percent of Medicare. The key question is whether changes in Medicaid PCP supply are likely to be consistent with changes in Medicaid enrollment—in other words, will states with the largest Medicaid enrollment increase also see the largest increases in Medicaid PCP supply?
Back to Top
How the Study Was Done
![]() onsistent with the definition used in the PPACA, primary care physicians are defined in this study to include physicians who specialize in general internal medicine, family practice or general pediatrics. The study classified states into three groups—low-, medium-, and high-PCP states—based on the ratio of PCPs to the nonelderly U.S. population in 2008, using the Health Resources and Services Administration (HRSA) Area Resource File. Low-, medium-, and high-PCP states were determined based on the distribution of the U.S. population into these groups (i.e. 25% of the U.S. population are in low-PCP states, and 25% are in high-PCP states).
onsistent with the definition used in the PPACA, primary care physicians are defined in this study to include physicians who specialize in general internal medicine, family practice or general pediatrics. The study classified states into three groups—low-, medium-, and high-PCP states—based on the ratio of PCPs to the nonelderly U.S. population in 2008, using the Health Resources and Services Administration (HRSA) Area Resource File. Low-, medium-, and high-PCP states were determined based on the distribution of the U.S. population into these groups (i.e. 25% of the U.S. population are in low-PCP states, and 25% are in high-PCP states).
Medicaid PCP supply in each state group is based on estimates of the percentage of PCPs reporting they were accepting all or most new Medicaid patients, using HSC’s nationally representative 2008 Health Tracking Physician Survey (see Data Source and Methods). These percentages are then applied to the total number of PCPs in each of the three groups of states to obtain estimates of the total number of PCPs accepting Medicaid patients. A ratio of the number of Medicaid PCPs to the total number of Medicaid enrollees within each of the three groups is computed, using state estimates of the number of nonelderly persons enrolled in Medicaid for 2008 from Kaiser State Health Facts.
The effect of increasing Medicaid reimbursement rates on Medicaid PCP supply is based on a regression model that links state-level Medicaid reimbursement rates for primary care services (as a percentage of Medicare rates) to the physician survey data, and that also accounts for other differences in physician and patient characteristics and health care market factors. The regression model is used to simulate the percent of PCPs who would accept all or most new Medicaid patients if reimbursement levels were equal to 100 percent of Medicare. These simulated percentages are then applied to the total number of PCPs within each state group to estimate the potential impact of Medicaid reimbursement increases on Medicaid PCP supply.
Back to Top
Geographic Variation in PCP Supply
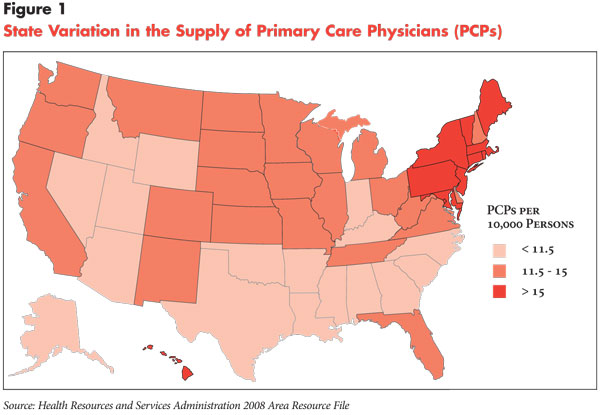
![]() rimary care physician supply varies considerably by region of the country. States with the highest levels of PCP supply—relative to the population—are concentrated almost entirely in the Mid-Atlantic and Northeast, while states with the lowest PCP supply are concentrated largely in the South and Mountain West (see Figure 1). In part, this reflects the higher levels of PCP supply in urban areas—which are more prevalent in the Northeast—while small towns and rural areas are more prevalent in southern and western states.
rimary care physician supply varies considerably by region of the country. States with the highest levels of PCP supply—relative to the population—are concentrated almost entirely in the Mid-Atlantic and Northeast, while states with the lowest PCP supply are concentrated largely in the South and Mountain West (see Figure 1). In part, this reflects the higher levels of PCP supply in urban areas—which are more prevalent in the Northeast—while small towns and rural areas are more prevalent in southern and western states.
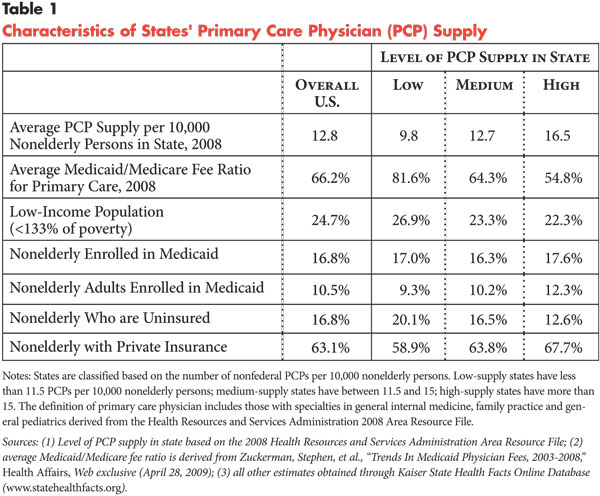
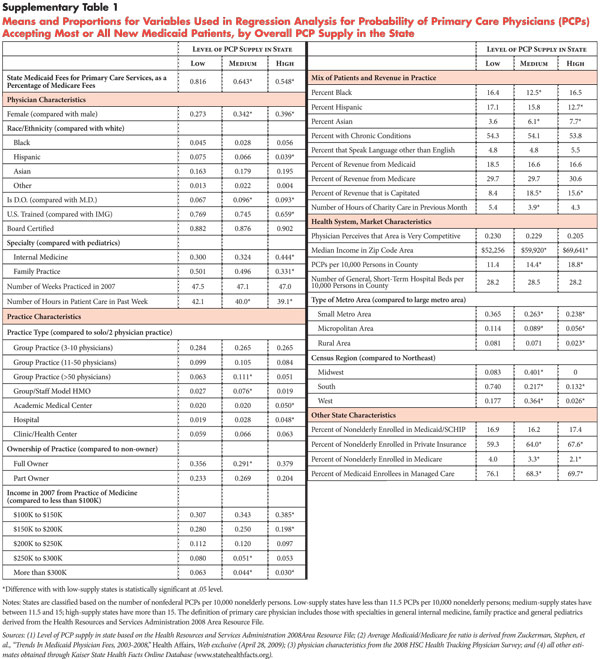
Low- and high-PCP states also vary by state Medicaid program characteristics. Importantly, Medicaid reimbursement rates for primary care—as a percentage of Medicare rates—are much higher on average in low-PCP states (81.6%) compared to high-PCP states (54.8%) (see Table 1). The low-PCP states include six—Idaho, Oklahoma, Wyoming, Alaska, North Carolina and Arizona—with reimbursement rates that are 95 percent of Medicare or higher.
Currently, there is little or no difference between high- and low-PCP states in terms of the proportion of the nonelderly population enrolled in Medicaid, despite the fact that low-PCP states have a higher proportion of poor and low-income persons (less than 133% of poverty) compared to high-PCP states. Low-PCP states tend to have more restrictive Medicaid eligibility, as exemplified by the fact that only one—Arizona—currently allows Medicaid eligibility for at least some parents or childless adults with incomes above 100 percent of poverty. By contrast, all but one—Pennsylvania—of the high-PCP states have expanded Medicaid eligibility up to or beyond 100 percent of poverty to at least some parents or childless adults. Low-PCP states also tend to have more uninsured residents and fewer privately insured persons.
Acceptance of New Medicaid Patients
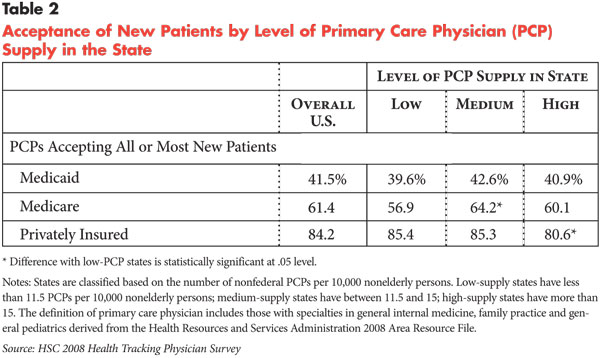
![]() ationally, 42 percent of primary care physicians were accepting all or most new Medicaid patients in 2008 (see Table 2).This is considerably lower than the 61 percent of PCPs accepting all or most new Medicare patients and the 84 percent accepting all or most privately insured patients. On average, there is no variation in Medicaid acceptance rates among PCPs depending on the overall level of PCP supply in the state. This is unexpected given that low-PCP states have substantially higher Medicaid reimbursement for primary care on average compared to high-PCP states.
ationally, 42 percent of primary care physicians were accepting all or most new Medicaid patients in 2008 (see Table 2).This is considerably lower than the 61 percent of PCPs accepting all or most new Medicare patients and the 84 percent accepting all or most privately insured patients. On average, there is no variation in Medicaid acceptance rates among PCPs depending on the overall level of PCP supply in the state. This is unexpected given that low-PCP states have substantially higher Medicaid reimbursement for primary care on average compared to high-PCP states.
Lack of variation in PCP acceptance of new Medicaid patients among the three groups of states reflects two factors:
- reimbursement rates have a relatively modest effect on PCP participation in Medicaid when accounting for other differences in physician and practice characteristics, and;
- there are a number of other factors, such as practice type and ownership, that increase Medicaid participation among PCPs, and some of these factors are more prevalent in states with high-PCP supply.
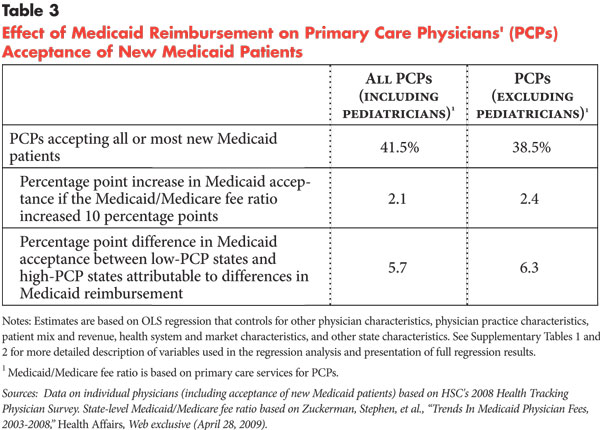
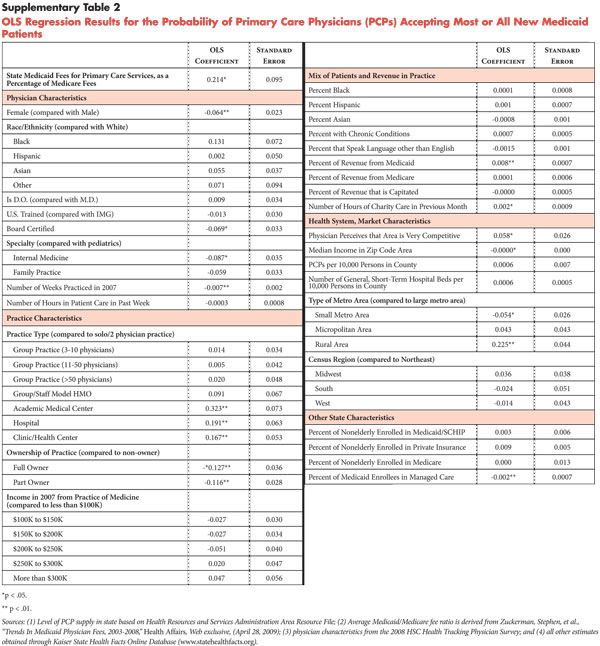
Regression analysis is used to examine the effects of Medicaid reimbursement rates on PCP acceptance of Medicaid patients, while accounting for differences in physician practice, patient and health care market characteristics. These results show that higher Medicaid reimbursement rates are associated with a greater probability of PCPs accepting all or most new Medicaid patients, although the effects are relatively modest. For PCPs, a 10-percentage point increase in the Medicaid/Medicare fee ratio for primary care is associated with only a 2.1-percentage-point increase in PCP Medicaid patient acceptance (see Table 3). Excluding pediatricians, the effect of reimbursement on Medicaid acceptance is slightly higher.
The modest effect of Medicaid reimbursement levels reflect in part the importance of other factors that affect PCP decisions to accept Medicaid patients. For example, independent of reimbursement levels, acceptance of Medicaid patients is more likely among male PCPs; those practicing in hospitals and academic medical centers rather than solo or group practices; those employed by their practices vs. being full or part owners of their practices; and PCPs practicing in lower-income and rural areas. Some of these factors offset low reimbursement rates because they are more prevalent in states with higher-PCP supply, such as the percentage of PCPs who are affiliated with academic medical centers and hospitals.
Even if PCPs were similar on these other factors, Medicaid acceptance would only be modestly higher in low-PCP states (i.e. states that have higher reimbursement levels). In other words, if PCPs in low-supply states were similar to PCPs in high-supply states on all measured factors other than level of reimbursement, Medicaid acceptance would be 5.7 percentage points higher in low-PCP states compared to high-PCP states.10
Back to Top
State Differences in Relative Supply of Medicaid PCPs
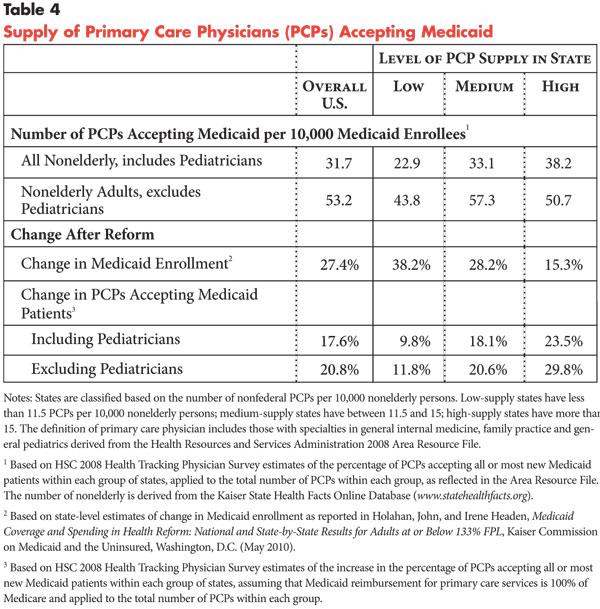
![]() ombining data on the number of PCPs with the percentage accepting Medicaid patients within each of the three groups of states shows that there are 38.2 PCPs accepting Medicaid patients for every 10,000 nonelderly enrollees in high-PCP states, compared to 22.9 PCPs in low-PCP states. In other words, Medicaid PCP supply is 1.67 times higher in high-supply states compared to low-supply states (see Table 4). Since there is little variation in Medicaid acceptance rates among PCPs across the three groups, this difference is almost entirely a result of differences in the overall supply of PCPs.
ombining data on the number of PCPs with the percentage accepting Medicaid patients within each of the three groups of states shows that there are 38.2 PCPs accepting Medicaid patients for every 10,000 nonelderly enrollees in high-PCP states, compared to 22.9 PCPs in low-PCP states. In other words, Medicaid PCP supply is 1.67 times higher in high-supply states compared to low-supply states (see Table 4). Since there is little variation in Medicaid acceptance rates among PCPs across the three groups, this difference is almost entirely a result of differences in the overall supply of PCPs.
However, these differences are narrowed considerably when focusing only on Medicaid PCP capacity for nonelderly adults—excluding pediatricians and children less than age 18 from the calculations. Medicaid physician supply for adults is 1.16 times higher in high-PCP states compared to low-PCP states and is highest in medium-PCP states (57.3 PCPs per 10,000 nonelderly adult Medicaid enrollees). The smaller difference when including only adult Medicaid enrollees reflects the larger number of adult Medicaid enrollees in high-PCP states—where eligibility standards are more generous—compared to low-PCP states where Medicaid eligibility for adults above the poverty level is rare.
Potential Effects of Health Reform
![]() ore restrictive Medicaid eligibility standards in low-PCP states mean that they will potentially experience a much larger increase in Medicaid enrollment when eligibility for adults expands to 133 percent of poverty, compared to states with higher-PCP supply. Based on state-level projections by the Urban Institute, Medicaid enrollment under the reform law’s eligibility expansion could increase as much as 38 percent in low-PCP states on average, compared to 15 percent in high-PCP states. Most of these new enrollees will be adults.
ore restrictive Medicaid eligibility standards in low-PCP states mean that they will potentially experience a much larger increase in Medicaid enrollment when eligibility for adults expands to 133 percent of poverty, compared to states with higher-PCP supply. Based on state-level projections by the Urban Institute, Medicaid enrollment under the reform law’s eligibility expansion could increase as much as 38 percent in low-PCP states on average, compared to 15 percent in high-PCP states. Most of these new enrollees will be adults.
Ironically, the fact that Medicaid reimbursement for primary care is already relatively high in low-PCP states means that the temporary increase in Medicaid reimbursement rates for primary care will have less impact on increasing the supply of Medicaid PCPs in these states compared to high-PCP states. This is demonstrated by using the state variation in Medicaid reimbursement rates and the same regression analysis described previously to simulate the increase in PCP acceptance of Medicaid patients if reimbursement for primary care is increased to 100 percent of Medicare. The results show that for low-PCP states, an increase from the current average of 81.6 percent to 100 percent of Medicare rates will result in only about a 10-percent increase in Medicaid PCP supply. This means that for states that currently have a low supply of PCPs, the percent increase in Medicaid enrollment under the reform law will be almost four times greater than the percent increase in Medicaid PCP supply.
In contrast, for high-PCP states, an increase from the current average of 54.8 percent to 100 percent of Medicare rates will result in a 23.5-percent increase in Medicaid PCP supply, gains that will likely exceed the increase in Medicaid enrollment. This reflects both low average reimbursement rates in high-PCP states—which means the effect of the reimbursement increase will be greater—and the higher number of adults who are currently eligible for and enrolled in Medicaid. In sum, Medicaid PCP supply will likely increase the most in states that already have the largest PCP supply relative to the Medicaid population, while shortages of PCPs for Medicaid enrollees are likely to grow even worse in states that already have low Medicaid PCP supply.
For the roughly half of the U.S. population who currently live in medium-PCP states, gains in enrollment will also exceed increases in Medicaid PCP supply in percentage terms, although the gap is not as large as for low-PCP states. Thus, most of the nation will likely observe Medicaid enrollment increases that exceed increases in Medicaid PCP supply.
Back to Top
Supply of Specialists
![]() tate variation in the supply of medical and surgical specialists for Medicaid is similar to PCP supply. States that have high overall supply of PCPs also have a greater supply of specialists (see Table 5). Unlike for PCPs, however, a higher percentage of specialists (58.4%) in low-PCP states accept most or all new Medicaid patients, compared to medium- and high-PCP states—where 48.5 percent and 50.6 percent of specialists, respectively, accept most or all new Medicaid patients. Nevertheless, the supply of specialists accepting Medicaid patients relative to the number of Medicaid enrollees is still much higher in high-PCP states (92.1 specialists per 10,000 nonelderly Medicaid enrollees compared to 59.5 in low-PCP states).
tate variation in the supply of medical and surgical specialists for Medicaid is similar to PCP supply. States that have high overall supply of PCPs also have a greater supply of specialists (see Table 5). Unlike for PCPs, however, a higher percentage of specialists (58.4%) in low-PCP states accept most or all new Medicaid patients, compared to medium- and high-PCP states—where 48.5 percent and 50.6 percent of specialists, respectively, accept most or all new Medicaid patients. Nevertheless, the supply of specialists accepting Medicaid patients relative to the number of Medicaid enrollees is still much higher in high-PCP states (92.1 specialists per 10,000 nonelderly Medicaid enrollees compared to 59.5 in low-PCP states).
Medicaid reimbursement levels for specialists will not be affected under health reform, which means the supply of specialists accepting Medicaid is unlikely to change substantially. The number of specialists accepting Medicaid patients relative to the number of Medicaid enrollees will decrease in all states but will probably decrease the most in low-PCP states given higher potential growth in the Medicaid population.
Back to Top
Policy Implications
![]() o address potential PCP shortages for Medicaid patients as eligibility expands, the reform law also calls for a temporary increase in Medicaid reimbursement rates for primary care. However, states that currently have the fewest number of PCPs relative to the population—primarily in the South and Mountain West—already have Medicaid reimbursement rates close to or exceeding Medicare rates and, therefore, will see relatively little impact from the increased Medicaid reimbursement rates. States with low-PCP supply also tend to have a high uninsured rate and few adults above the federal poverty line who are currently eligible for Medicaid, so these states will likely have the greatest enrollment increases—and demand for medical care—when the Medicaid eligibility expansions occur in 2014.
o address potential PCP shortages for Medicaid patients as eligibility expands, the reform law also calls for a temporary increase in Medicaid reimbursement rates for primary care. However, states that currently have the fewest number of PCPs relative to the population—primarily in the South and Mountain West—already have Medicaid reimbursement rates close to or exceeding Medicare rates and, therefore, will see relatively little impact from the increased Medicaid reimbursement rates. States with low-PCP supply also tend to have a high uninsured rate and few adults above the federal poverty line who are currently eligible for Medicaid, so these states will likely have the greatest enrollment increases—and demand for medical care—when the Medicaid eligibility expansions occur in 2014.
A limitation of this analysis is that the simulated rate increases assumed a permanent increase in Medicaid reimbursement relative to Medicare, while the rate increases specified in the law are limited to 2013 and 2014. The temporary nature of the rate increase may limit the incentive for more physicians to accept Medicaid patients, in which case the increase in Medicaid PCP supply will be less than shown in this analysis. While the federal government and/or states have the option of extending these increases beyond 2014, budgetary pressures and uncertainty about what shortages will develop when reform is implemented are likely to preclude decisions on extensions.
Other PPACA provisions are designed to increase the availability of primary care. For example, the law includes a 10 percent bonus in Medicare payments from 2011 to 2016 to PCPs for certain services. The law also includes incentives for medical students to choose primary care specialties through new scholarship and loan repayment programs and to practice at least initially in an underserved area. Under another PPACA provision, the U.S. Department of Health and Human Services (HHS) could choose to address geographic PCP disparities by redistributing unfilled hospital residency positions for training primary care physicians and general surgeons. Addressing geographic disparities in primary care supply also could be included in the criteria that HHS develops to award grants to hospitals and medical schools for developing training programs in primary care specialties, including a program designed to recruit and train students likely to work in rural, underserved areas.
Efforts to increase the supply of nurse practitioners and other mid-level practitioners—such as through increases in the Nursing Student Loan Program and funding for nurse-managed health clinics—also are included in the law to address looming shortages in primary care. If nurse practitioners are to be used to address shortages in primary care, then it will be important to resolve issues around their scope of practice, or what they can do without direct involvement or supervision of a physician.
Currently, most southern states with low-PCP supply have some of the strongest restrictions on scope of practice for nurse practitioners—for example, they are not allowed to diagnose, treat or prescribe medicines to patients without the involvement of physicians, according to Kaiser State Health Facts. Such restrictions are likely to limit the ability of nurse practitioners to address primary care shortages, especially in rural areas that may have few or no physicians, although severe access problems may ultimately induce these states to ease scope-of-practice restrictions.
Nevertheless, it is doubtful that such measures alone will alleviate the shortages likely to be encountered in states with low-PCP supply and the largest increase in Medicaid enrollment. Low-PCP supply in these states likely developed over a long period as a consequence of their comparatively low family incomes, high uninsured rates, fewer academic medical centers and fewer large cities, which made these states less attractive to physicians relative to the more-affluent and urbanized states of the Northeast. Prior research has shown that economic growth in an area increases the supply of physicians, but that such increases in supply lag economic growth by about 10 years.11 While the PPACA may not directly increase economic growth, the large expansions in health insurance coverage in low-PCP states may have a comparable effect on the supply of physicians, making these states more attractive to physicians and other health care providers over time. Thus, the wide and growing disparities in PCP supply across states suggested by this study’s results may moderate over time as health reform takes effect.
The measures of PCP acceptance of Medicaid patients in this analysis did not distinguish between fee-for-service and managed care patients. Managed care enrollment among Medicaid enrollees has increased to about 70 percent for all types of managed care (including primary care case management) and 46 percent for those in a comprehensive managed care plan. The analysis accounted for the overall amount of physicians’ practice revenue based on capitated payments, as well as state differences in Medicaid managed care penetration, but there was no information in the survey data and no prior research on whether PCPs are more or less likely to accept Medicaid managed care vs. fee-for-service patients.
Shortages of PCPs willing to treat Medicaid patients could make it difficult for Medicaid managed care plans to recruit sufficient numbers of PCPs into their networks, although broader efforts to increase the integration and coordination of primary and specialty care may offset some of the shortages. For example, other research has shown that some PCPs do not accept Medicaid patients because they have difficulty obtaining specialty referrals, which a more integrated and coordinated approach to care delivery may mitigate.12 More integrated and organized systems of care also can decrease Medicaid administrative burdens, which physicians also frequently cite as a reason for not accepting Medicaid patients.
Managed care plans also have flexibility to pay PCPs at higher rates than they would receive under fee-for-service Medicaid—a tool plans can use to recruit PCPs and other physicians into their networks. Shifting to new payment models, such as performance-based incentives and global payment—as some states already are experimenting with—may also permit higher payments to physicians without necessarily increasing program costs if successful, while at the same time improving patient access to medical homes and continuity of care.
As increases in reimbursement rates alone cannot increase the supply of Medicaid PCPs to levels necessary for the likely growth in the Medicaid population, combining payment reforms with delivery system reforms will ultimately be essential to meet the long-term challenges of increased demand and limited supply.
Back to Top
Notes
Back to Top
Data Source
This Research Brief presents findings from the HSC 2008 Health Tracking Physician Survey, a nationally representative mail survey of U.S. physicians providing at least 20 hours per week of direct patient care. The sample of physicians was drawn from the American Medical Association (AMA) master file and included active, nonfederal, office- and hospital-based physicians. Residents and fellows were excluded, as well as radiologists, anesthesiologists and pathologists. The survey includes responses from more than 4,700 physicians, and the response rate was 62 percent. The sample used for this analysis includes 1,748 physicians who identified their primary specialty as general internal medicine, family practice or general pediatrics.
In addition, physicians who practice on staff at a hospital or in an emergency room were excluded from the sample, but physicians in an office-based practice owned by a hospital or academic medical center were included. Estimates from this survey should not be compared to estimates from HSC’s previous Community Tracking Study physician surveys because of changes in the survey administration mode from telephone to mail, question wording, skip patterns, sample structure and population represented. More detailed information on survey content and methodology can be found at www.hschange.org.
Classification of states based on the supply of primary care physicians. States were initially classified into three groups based on their overall number of nonfederal PCPs relative to the size of the nonelderly population in 2008. Consistent with the definition used in the PPACA, PCPs include physicians who indicate their specialty as general internal medicine, family practice or general pediatrics. Thresholds for determining low-, medium-, and high- PCP-supply states are based on the distribution of the U.S. population. Low-PCP states comprise approximately 25 percent of the U.S. population, while high-PCP states comprise another 25 percent of the population. Medium-PCP states comprise about half of the U.S. population. Information on state-level-PCP supply for 2008 is based on the Area Resource File maintained by HRSA.
Medicaid PCP supply within each of the three groups was based on estimates of the percentage of PCPs who reported that they were accepting all or most new Medicaid patients in the 2008 Health Tracking Physician Survey. The survey does not permit state-specific estimates of the percentage of physicians accepting most or all new Medicaid patients. However, the sample of physicians is representative of the nation and groups of states, including the low-, medium-, and high-PCP states as previously defined. Estimates of Medicaid acceptance within each of the groups reflect the weighted average for that group.
The percentage of PCPs accepting Medicaid patients based on the survey data is then applied to the total number of PCPs within each group (as previously described) to obtain the total number of PCPs accepting Medicaid patients. A ratio of the number of Medicaid PCPs (i.e. PCPs accepting Medicaid patients) to the total number of Medicaid enrollees within each of the three groups is computed, using state estimates of the number of nonelderly persons enrolled in Medicaid for 2008 from Kaiser State Health Facts.
Increase in Medicaid acceptance by PCPs based on increase in reimbursement rates. Determining the potential increase in the number of PCPs accepting Medicaid patients when reimbursement is increased to 100 percent of Medicare is based on multivariate regression analysis. Consistent with prior research, the regression model assumes that willingness to accept all or most new Medicaid patients on the part of PCPs is a function of state-level Medicaid reimbursement rates for primary care services (as a percentage of Medicare rates) as well as other physician, practice and patient characteristics; the relative size of the Medicaid population in the state; and health care market factors (see Supplementary Tables 1 and 2 for a complete set of variables and results).7 The results for the effect of state-level Medicaid reimbursement rates for primary care services are then used to simulate the marginal percentage point increase in Medicaid acceptance for each of the three PCP-supply groups assuming that Medicaid reimbursement rates for primary care services are equal to Medicare.8
For example, to simulate the effect of increasing reimbursement rates to 100 percent of Medicare in low-PCP states, the difference between 100 percent and the current average reimbursement rate for low-PCP states (81.6 percent) is applied to the regression coefficient for Medicaid reimbursement rate (0.214). The result reflects the percentage point increase in Medicaid acceptance rates (3.9) among PCPs in low-PCP states if Medicaid reimbursement rates were increased to 100 percent of Medicare. The simulated percent of PCPs accepting Medicaid patients is then applied to the total number of PCPs in low-PCP states to derive an estimate of the number of PCPs accepting Medicaid if reimbursement rates were increased to 100 percent of Medicare.
Estimates of the effects of reimbursement on Medicaid acceptance are computed for all PCPs—general internal medicine, family practice and pediatricians—and with pediatricians excluded. Since the vast majority of the new Medicaid enrollees under the eligibility expansions will be adults, it’s important to assess the effects of reimbursement changes after excluding pediatricians. Estimates of the change in Medicaid eligibility and enrollment after implementation of the PPACA are based on projections by the Urban Institute.9
Funding Acknowledgement:
This research was supported by the Robert Wood Johnson Foundation.
Back to Top
Supplementary Tables
RESEARCH BRIEFS are published by the Center for Studying Health System
Change.
600 Maryland Avenue, SW, Suite 550
Washington, DC 20024-2512
Tel: (202) 484-5261
Fax: (202) 484-9258
www.hschange.org