Health and Wellness: The Shift from Managing Illness to Promoting Health
Issue Brief No. 121
June 2008
Debra A. Draper, Ann Tynan, Jon B. Christianson
Despite an acknowledged lack of evidence of investment payoff, health plan initiatives to promote health and wellness are now commonplace, according to findings from the Center for Studying Health System Change’s (HSC) 2007 site visits to 12 nationally representative metropolitan communities. Much of the impetus has come from employers—primarily large employers—that are incorporating health and wellness activities into benefit designs that place more responsibility on employees for health care decisions and costs. Health plans now offer a range of health and wellness activities, including traditional worksite health fairs, screenings and educational seminars; access to behavior modification programs, such as weight management and smoking cessation; and online tools, including health risk assessments. Engaging enrollees in these activities, however, is challenging because participation typically is voluntary. Another barrier is employee privacy concerns. More health plans and employers are turning to financial incentives to secure greater participation. Ultimately, however, the credibility of health and wellness activities as mechanisms to improve health and contain costs is dependent on evidence demonstrating their clinical and financial effectiveness, as well as consumers’ acceptance and validation of their legitimacy.
- Health and Wellness Initiatives Part of Broader Consumerism Strategy
- Plans Build Capacity
- Range of Activities
- Enrollee Engagement
- Investment Payoff
- Implications
- Notes
- Data Source
Health and Wellness Initiatives Part of Broader Consumerism Strategy
![]() ueled in part by heightened awareness of the nation’s growing
obesity crisis, health plan initiatives to promote health and wellness are now
commonplace across the country, according to findings from HSC’s 2007 site
visits to 12 nationally representative metropolitan communities (see Data Source).
Much of the momentum has come from employers—predominantly large employers—looking
for effective long-term strategies to address rising costs and to support their
broader consumer-based strategy of giving employees more responsibility for
health care decisions and costs. As a Phoenix health plan executive commented,
“Overall health is not improving, although consumers’ appetite for
health care continues to increase. Employers are concerned about affordability…[they]
want to offer coverage, but they also want to engage their employees differently.”
ueled in part by heightened awareness of the nation’s growing
obesity crisis, health plan initiatives to promote health and wellness are now
commonplace across the country, according to findings from HSC’s 2007 site
visits to 12 nationally representative metropolitan communities (see Data Source).
Much of the momentum has come from employers—predominantly large employers—looking
for effective long-term strategies to address rising costs and to support their
broader consumer-based strategy of giving employees more responsibility for
health care decisions and costs. As a Phoenix health plan executive commented,
“Overall health is not improving, although consumers’ appetite for
health care continues to increase. Employers are concerned about affordability…[they]
want to offer coverage, but they also want to engage their employees differently.”
Health and wellness initiatives also offer health plans a way to reposition themselves with employers and enrollees, alike. As an Indianapolis health plan executive said, “Our value proposition has to be built around how we are going to help you manage health care costs. This involves not just managing illness, but where health care companies have been [deficient] in the past is in how often they talk to healthy members. They only talked to members when they had a claims issue. We are trying to build an organization that is interactive with all members, not just the ones who are sick.”
Employers hope that health and wellness activities will reduce absenteeism and
improve productivity, as well as avoid major, costly medical events. A recent
American Hospital Association report, for example, estimated that three chronic
diseases—asthma, diabetes and hypertension—result in 164 million days
of absenteeism each year, costing employers $30 billion.1 As a northern New
Jersey plan medical director surmised, “When employers look at employees
and see many are obese and understand the implications for diabetes and cardiovascular
disease, they start keeping an eye on wellness.”
Back to Top
Plans Build Capacity
![]() ncreasingly, health plans are building, acquiring or enhancing capabilities to deliver health and wellness services, in part because they “found themselves losing the business to [non-health plan] vendors,” according to a Seattle benefits consultant. Plans are emphasizing to their employer customers the value of integrating health and wellness activities with other care management efforts dependent on plans’ claims data.
ncreasingly, health plans are building, acquiring or enhancing capabilities to deliver health and wellness services, in part because they “found themselves losing the business to [non-health plan] vendors,” according to a Seattle benefits consultant. Plans are emphasizing to their employer customers the value of integrating health and wellness activities with other care management efforts dependent on plans’ claims data.
Across the 12 HSC communities, health plans are packaging, branding and marketing health and wellness activities as a way of differentiating themselves in the market. Often these activities are marketed as a key component of a comprehensive approach to care management. As a Cleveland plan medical director noted, “All plans offer these things. But it comes down to how you package these tools so that it looks like what you’re doing really works, try to differentiate [yourself].”
Back to Top
Range of Activities
![]() ealth and wellness activities are premised on the idea that healthier people will use fewer medical resources and be more productive. These activities target enrollees irrespective of disease status or health utilization and are intended to encourage the pursuit of healthy behaviors, including supporting people who are interested in making lifestyle changes. Health and wellness initiatives go beyond screening activities, such as mammograms and colonoscopies that detect disease, and differ from disease management and case management interventions, which are used once a disease is diagnosed.
ealth and wellness activities are premised on the idea that healthier people will use fewer medical resources and be more productive. These activities target enrollees irrespective of disease status or health utilization and are intended to encourage the pursuit of healthy behaviors, including supporting people who are interested in making lifestyle changes. Health and wellness initiatives go beyond screening activities, such as mammograms and colonoscopies that detect disease, and differ from disease management and case management interventions, which are used once a disease is diagnosed.
While many of the health and wellness activities plans offer are not new, what has changed is the heightened awareness and intensity of the initiatives. As a Boston plan executive described the evolution, “In the early days, health and wellness activities were nice to have. We used to do a lot of on-site health fairs. Now health and wellness are key components of programs for employers and this is a different trend. Even in the media, there seems to be heightened awareness of lifestyle and the impact of eating and exercise.”
In addition to health and wellness activities provided at the worksite, such as health fairs, educational seminars and screenings for such conditions as high-blood pressure and cholesterol levels, plans also are focusing on providing enrollees access to behavior modification programs to improve their health. These programs typically focus on weight management, smoking cessation and fitness. For example, a northern New Jersey plan has a healthy eating program that encourages enrollees to work with their primary care physicians to set and monitor weight-loss goals. A Cleveland plan works with a publicly funded tobacco-use prevention program to help fund the costs of nicotine replacement therapy and smoking cessation counseling for enrollees. Plans sometimes use health coaches to work individually with enrollees to provide additional support and encouragement to help them reach their goals.
One of the more notable developments across the 12 HSC communities is the growing interest in and use of health risk assessments, which have become more sophisticated and accessible through information technology improvements. A health risk assessment is a questionnaire, often available online, that collects information provided by the enrollee about personal and family medical history, current diagnoses and symptoms, use of preventive and screening services, and lifestyle behaviors, such as diet, physical activity, and tobacco and alcohol use. Based on this information, enrollees may be encouraged to participate in particular health and wellness activities or to visit their physician for a potentially acute problem. The information also is used to predict health risk, including the identification of enrollees with, for example, diabetes who may benefit from more intensive interventions, such as disease management or case management. If not appropriately treated and monitored, conditions like diabetes can result in increased utilization of health care services and costs.
Back to Top
Enrollee Engagement
![]() ngaging enrollees is challenging because participation in health and wellness activities typically is voluntary. Most respondents believed some type of incentive is needed to engage people—not only to get them involved initially, but also to encourage them to actually improve their health. Where incentives exist, they tend to vary widely in size and design. They include, for example, small cash payments for the completion of a health risk assessment, gift cards, gym membership discounts, and reimbursement for weight management programs, such as Weight Watchers.
ngaging enrollees is challenging because participation in health and wellness activities typically is voluntary. Most respondents believed some type of incentive is needed to engage people—not only to get them involved initially, but also to encourage them to actually improve their health. Where incentives exist, they tend to vary widely in size and design. They include, for example, small cash payments for the completion of a health risk assessment, gift cards, gym membership discounts, and reimbursement for weight management programs, such as Weight Watchers.
Incentives for participation in health and wellness activities that are incorporated in consumer-directed health plans (CDHPs), however, are often larger.2 For example, an Indianapolis health plan uses a range of incentives in its CDHP product to encourage participation in health and wellness activities. Up to $100 is deposited in enrollees’ health spending accounts when they complete a health risk assessment. An additional $100 is deposited if enrollees sign up for a personal health-coaching program, and they can earn another $250 contribution for completing a weight loss or smoking cessation program. As the plan marketing executive noted, “When you offer a CDHP, if you don’t complement it with wellness, it is just cost shifting. It is critical that every employer offering a CDHP complements it with a very robust wellness program. They go hand-in-hand with each other. We can’t expect somebody to be a smarter consumer of health care and living that in terms of lifestyle and need, if we’re not helping consumers take care of themselves.”
Plans typically use incentives to encourage participation in health and wellness activities rather than penalizing those who do not participate. As a Greenville plan medical director said, “At this point, we don’t see anybody creating sticks or any type of negative processes if they don’t participate. It’s more like a reward if they do.” But health plan and employer respondents in several communities noted that, increasingly, the discussion is shifting away from how to encourage participation to applying incentives to results. UnitedHealthcare, for example, offers a product to employers where the employee can reduce the size of the plan deductible through verified absence of smoking and meeting objectives for body-mass index and blood-pressure and cholesterol levels.3 Employers also are considering instituting premium differentials for employees based on whether they participate in health and wellness activities, but recent regulatory guidelines issued by the U.S. Department of Labor limit the differentials.4 The threat by an Indianapolis health system to move in this direction reportedly met with stiff employee resistance.5
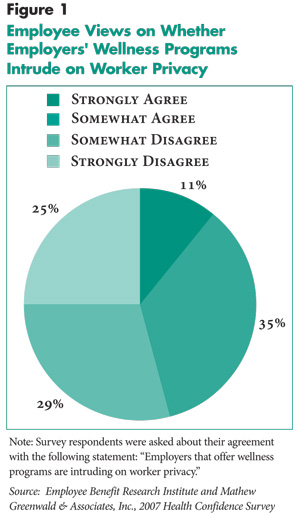
There also are concerns about health and wellness activities impinging on employee privacy, similar to findings from the 2007 Health Confidence Survey conducted by the Employee Benefit Research Institute and Mathew Greenwald & Associates, Inc. In this survey, nearly one in two employees believed that employers who offer wellness programs are intruding on worker privacy (Figure 1). As a large Phoenix employer noted, “Some people are worried about privacy, how the data they report on the health risk assessment will be used.” A Miami benefits consultant questioned the validity of employee-provided information on health risk assessments, especially if employees believe employers will use the information to reduce benefits, for example. Cognizant of these concerns, several health plan respondents reported that they had implemented systems to assure enrollees that their privacy is protected.
Back to Top
 |
Investment Payoff
![]() unding for health and wellness activities comes from several sources. For fully insured products, the cost typically is incorporated into the premium, while self-insured employers typically pay a fee to the plan administrator. Despite growing enthusiasm for health and wellness activities, the investment payoff has been difficult to demonstrate. A benefits consultant in northern New Jersey described the challenge, “The costs are difficult to get at. Sometimes it’s hard to get at productivity. We’re moving that way, but it’s going to be slow going. There is recognition that a healthier workforce leads to less spending and more productivity, but it’s hard to prove. The challenge is there is no control group to measure it against. There is no way to prove what health spending would have been in the absence of change.”
unding for health and wellness activities comes from several sources. For fully insured products, the cost typically is incorporated into the premium, while self-insured employers typically pay a fee to the plan administrator. Despite growing enthusiasm for health and wellness activities, the investment payoff has been difficult to demonstrate. A benefits consultant in northern New Jersey described the challenge, “The costs are difficult to get at. Sometimes it’s hard to get at productivity. We’re moving that way, but it’s going to be slow going. There is recognition that a healthier workforce leads to less spending and more productivity, but it’s hard to prove. The challenge is there is no control group to measure it against. There is no way to prove what health spending would have been in the absence of change.”
Several health plan respondents also said that it takes at least three to five years to have sufficient information to determine return on investment. Because many of the health and wellness activities in existence today have only been introduced recently and not yet evaluated, there is little credible evidence regarding return on investment. Yet some plans and employers appear willing to invest in these activities, albeit on a generally limited basis, in the near term.
Some employers, particularly small firms or those with more transient workforces, are hesitant about investing in health and wellness activities. As a Phoenix plan executive noted, “Part of the issue for employers is how much of an investment to make considering employee turnover.” Despite a high turnover rate, one large national retailer headquartered in Phoenix incorporated health and wellness activities in a CDHP option that it began offering employees last year. According to an employer representative, the heath spending account is funded only if the employee completes a health risk assessment and participates in wellness activities.
Increasingly, employers are pressuring health plans (and non-health plan vendors) to demonstrate effectiveness, but much of the existing evidence is preliminary and often anecdotal. For example, early data from a smoking-cessation program offered by a Cleveland plan was reportedly positive, showing a short-term quit rate of 40-45 percent among a group of participating enrollees who used both nicotine replacement therapy and smoking cessation counseling. Health plans also are offering their own employees the health and wellness options they offer to the market more broadly. Several health plan respondents noted that this was important to establish the credibility of these efforts with potential employer customers.
Across the 12 communities, health plan and employer respondents frequently expressed the belief that investment in health and wellness activities is the right thing to do and is particularly important as employees assume more responsibility for health care decisions and costs. Several respondents noted that health and wellness activities seem to be particularly good ways to engage consumers—to heighten their awareness of what health care actually costs and to encourage more proactive participation in decisions about the use of services.
Back to Top
Implications
![]() mployers are increasingly looking to health and wellness initiatives to help support their shift to a broader consumer-based strategy of employees taking more responsibility for health care decisions and costs. These activities offer promise for engaging consumers more effectively—to help consumers be more aware, knowledgeable and thoughtful in making health and lifestyle choices, as well as the use of health care resources. But there are significant challenges that will determine how effective health and wellness activities ultimately are, including:
mployers are increasingly looking to health and wellness initiatives to help support their shift to a broader consumer-based strategy of employees taking more responsibility for health care decisions and costs. These activities offer promise for engaging consumers more effectively—to help consumers be more aware, knowledgeable and thoughtful in making health and lifestyle choices, as well as the use of health care resources. But there are significant challenges that will determine how effective health and wellness activities ultimately are, including:
- Engaging larger numbers of consumers to actively participate by using incentives that minimize resistance, best achieve the desired outcomes, and appropriately address consumers’ privacy concerns; and
- Demonstrating their effectiveness in improving, or at least maintaining health, including evidence of an investment payoff.
In the short term, it is likely that interest in health and wellness initiatives will gain momentum as employers continue to confront the pressure of rising health care costs. Longer term, however, the degree to which these initiatives are seen as credible health-improvement and cost-containment efforts will depend largely on developing evidence that initiatives are effective—clinically and financially. It also will depend on consumers’ acceptance and validation of their legitimacy.
Back to Top
Notes
Back to Top
Data Source
Every two years, HSC conducts site visits in 12 nationally representative
metropolitan communities as part of the Community Tracking Study to interview
health care leaders about the local health care market and how it has changed.
The communities are Boston; Cleveland; Greenville, S.C.; Indianapolis; Lansing,
Mich.; Little Rock, Ark.; Miami; northern New Jersey; Orange County, Calif.;
Phoenix; Seattle; and Syracuse, N.Y. The sixth round of site visits was conducted
between February and June 2007 with 453 interviews. In each community, representatives
from at least two of the largest health plans were interviewed. Health plan
representatives included the medical director, a marketing executive and a network
executive. Interviews also were conducted with benefit consultants, brokers
and representatives of at least two large employers.
Back to Top
ISSUE BRIEFS are published by the
Center for Studying Health System Change.
600 Maryland Avenue, SW, Suite 550
Washington, DC 20024-2512
Tel: (202) 484-5261
Fax: (202) 484-9258
www.hschange.org