
HSC Research Brief No. 20
May 2011
Joy M. Grossman, Ellyn R. Boukus, Dori A. Cross, Genna R. Cohen
Hoping to reduce medication errors and contain health care costs, policy makers are promoting electronic prescribing through Medicare and Medicaid financial incentives. Many e-prescribing systems provide electronic access to important information—for example, medications prescribed by physicians in other practices, patient formularies and generic alternatives—when physicians are deciding what medications to prescribe. However, physician practices with e-prescribing face challenges using these features effectively, according to a new qualitative study by the Center for Studying Health System Change (HSC) funded by the Agency for Healthcare Research and Quality (AHRQ).
While most of the 24 practices studied reported that physicians had access to patient formulary information, only slightly more than half reported physician access to patient medication histories, and many physicians did not routinely review these sources of information when making prescribing decisions. Study respondents highlighted two barriers to use: 1) tools to view and import the data into patient records were cumbersome to use in some systems; and 2) the data were not always perceived as useful enough to warrant the additional time to access and review them, particularly during time-pressed patient visits. To support generic prescribing, practices typically set their system defaults to permit pharmacist substitution of generics; many practices also used other tools to more proactively identify and select generic alternatives at the point of prescribing. Overall, physicians who more strongly perceived the need for third-party data, those in practices with greater access to complete and accurate data, and those with easier-to-use e-prescribing systems were more likely to use these features consistently.
![]() he federal government and other public- and private-sector entities are promoting e-prescribing because of the technology’s potential to improve health care quality and reduce health care spending in a variety of ways.1 The core feature of e-prescribing systems—the ability to write and store prescriptions electronically—may reduce medication errors, improve physician practice and pharmacy efficiency, and support care coordination by providing physicians with well-documented medication lists and pharmacists with legible and complete prescriptions. Moreover, direct electronic transmission of prescriptions from practice e-prescribing systems to pharmacy computer systems may help reduce errors related to manual entry at pharmacies and improve physician practice and pharmacy efficiency.
he federal government and other public- and private-sector entities are promoting e-prescribing because of the technology’s potential to improve health care quality and reduce health care spending in a variety of ways.1 The core feature of e-prescribing systems—the ability to write and store prescriptions electronically—may reduce medication errors, improve physician practice and pharmacy efficiency, and support care coordination by providing physicians with well-documented medication lists and pharmacists with legible and complete prescriptions. Moreover, direct electronic transmission of prescriptions from practice e-prescribing systems to pharmacy computer systems may help reduce errors related to manual entry at pharmacies and improve physician practice and pharmacy efficiency.
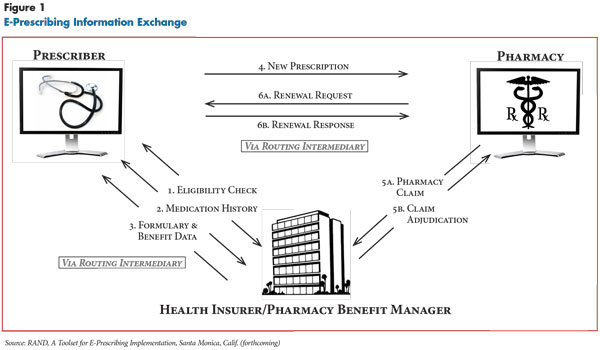
Many e-prescribing systems have features that give physicians access to difficult-to-get information from external sources that could potentially improve prescribing decisions, including patients’ medications prescribed by physicians in other practices, patient formularies and other prescription drug benefits, and generic medication alternatives (see box below and Figure 1 for more about accessing patient information from external sources). While there is limited research on the effects of physician access to such data through commercial e-prescribing systems, many experts believe that use of these features can improve quality of care and reduce costs.8
Specifically, while e-prescribing systems commonly capture all prescriptions written within a practice, physicians must rely on patients to provide information about medications prescribed by other providers. Access to a third-party source of a patient’s current and previous medications—in this case based on medication claims from health insurers and pharmacy benefit managers (PBMs)—might improve the accuracy of a patient’s medication list, potentially reducing errors, such as medication duplication, and providing physicians with information to help improve medication adherence. More comprehensive medication lists also may increase the value of electronic-alert features in many e-prescribing systems, such as notifications for drug-drug and drug-allergy interactions.
Similarly, providing physicians with easy access to up-to-date formulary and related benefit information could help improve efficiency by reducing pharmacy callbacks to physician practices to resolve coverage issues. And, easy access to generic alternatives to costly brand-name drugs through third-party medication database vendors may encourage physicians to prescribe more generics. Increasing on-formulary and generic prescribing could lower out-of-pocket costs for patients and overall medication expenditures and may improve adherence for patients who forgo medications because of cost.
These potential gains assume that physicians who e-prescribe have access to these features and use them. However, not all e-prescribing systems have these features, and even when the features are available, physician practices may not implement them or individual physicians may not use them.9 For example, a 2009 survey of physicians electronically routing prescriptions via Surescripts—the dominant electronic prescription transmission network in the United States—found that 62 percent had access to medication histories and 60 percent to formulary information.10 Of those physicians, 56 percent used medication histories most or all of the time, while 34 percent used formulary information most or all of the time. Available research suggests that missing, incomplete and inaccurate data limit the value to physicians of using e-prescribing systems to access medication histories and formulary information.11
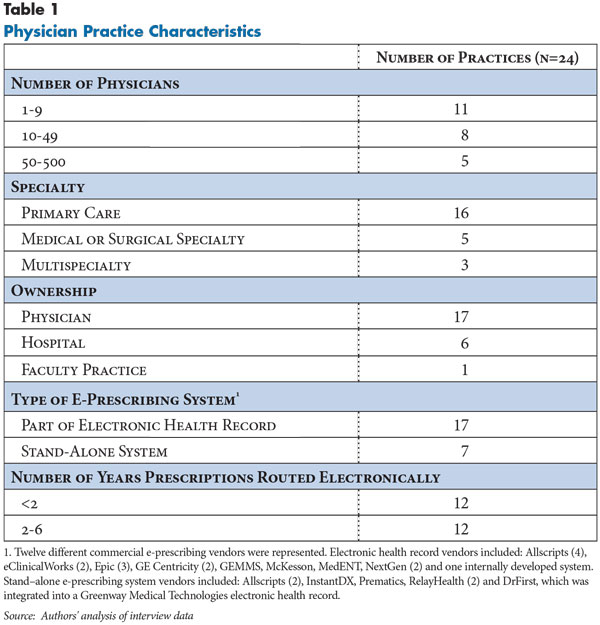
To better understand how physicians use e-prescribing systems to access external information, HSC researchers interviewed physicians and information technology (IT) staff in 24 physician practices (see Data Source). Two practices actively routing electronic prescriptions through Surescripts were selected in each of 12 nationally representative Community Tracking Study sites to capture variation in practice size, specialty and type of e-prescribing system (see Table 1).
The practices studied used products from 12 different vendors and one internally developed system. About 70 percent of practices used e-prescribing systems that were part of electronic health records (EHRs), while the remainder used stand-alone e-prescribing systems.12 Practices had varying degrees of experience routing electronic prescriptions, ranging from less than a year to more than five years, with more than two-thirds of practices estimating electronic routing of at least 70 percent of all prescriptions.
Accessing Patient Information from External SourcesProviding physicians with access to information from external sources via an e-prescribing system is a complex exchange of health information across multiple parties (see Figure 1). Surescripts is the main intermediary e-prescribing system vendors use to provide physicians with access to patient medication histories and formulary and benefit information from participating insurers and pharmacy benefit managers (PBMs). Other companies collect and sell formulary and benefit data, making products, such as Infoscan, available to vendors. If physicians wish to access a patient’s medication history or formulary information via Surescripts, they first must initiate an eligibility request to identify a patient’s health insurer or PBM. The request travels from the physician’s system via the e-prescribing vendor to Surescripts, which in turn transmits the request to participating health insurers and PBMs and then sends back a response. To match patients between these sources, a probabilistic algorithm relies on five patient identifiers sent from the physician’s e-prescribing system, including patient first and last names, date of birth, gender and zip code. If a match is made with the health insurer/PBM data, an eligibility key is returned that can link the patient to formulary information and medication history; otherwise an error message is sent. Upon physician request, eligibility information can then be used to match and return a patient’s medication history for up to the past two years based on adjudicated medication claims data.2 Participating health insurers/PBMs must provide medication name, strength, dosage form and date filled, with the option to include additional data such as prescriber, fill location, number of refills and whether or not the prescription was required to be dispensed as written. As part of the eligibility request, Surescripts requires physicians to complete a field indicating if patient consent to access the medication history has been obtained. In contrast to requests for patient eligibility and medication histories, which are real-time transactions, in the case of formularies, eligibility information is used to match a patient to information on the relevant drug plan stored in formulary files, which are downloaded to the practice’s computer periodically.3 These files are updated anywhere from daily to quarterly by participating health insurers and PBMs and then are available via Surescripts to e-prescribing vendors. Vendors are required to make files available weekly for practices to download. The timeliness of the information displayed to the physician depends on how frequently the different parties, including the practice, refresh the information. Health insurers and PBMs, at a minimum, indicate whether the drug selected by the physician is on formulary or not. Less commonly, additional data may be provided on copayment tiers, coverage limitations, on-formulary therapeutic alternatives and insurer/PBM requirements that physicians request prior authorization of insurance coverage before prescribing certain medications. Because these data are typically “representative” and are only provided for a subset of an insurer’s health plans, this information may not reflect the exact benefits under a patient’s specific policy.4 Commercial insurer and Medicaid participation in Surescripts is voluntary and not all payers provide information. In contrast, Medicare Part D plans are required to make all of the information available for e-prescriptions for Part D patients.5 While the overall number of participating payers continues to increase, as of 2009, only nine Medicaid plans were participating.6 In sum, Surescripts reported that prescription benefits and history information were available for more than 65 percent of patients in 2009 but with substantial geographic variation across the country. For example, the percentage of patients with available information in 2009 ranged from 47 percent to 90 percent in the 12 states where practices in this study were located (see Data Source).7 |
![]() nderstanding more fully what factors support or impede physician use of e-prescribing features is particularly important as physician adoption and use of e-prescribing accelerates in response to new federal incentive programs.13 The percentage of office-based physicians routing prescriptions via Surescripts more than doubled from 12.1 percent to 26 percent between 2008 and 2009, the year Medicare began paying bonuses to qualifying e-prescribing physicians under the Medicare Electronic Prescribing Incentive Program, established by the 2008 Medicare Improvements for Patients and Providers Act (MIPPA).14 The number of physician requests to Surescripts for patient medication histories and formulary information grew even more rapidly over the same period.
nderstanding more fully what factors support or impede physician use of e-prescribing features is particularly important as physician adoption and use of e-prescribing accelerates in response to new federal incentive programs.13 The percentage of office-based physicians routing prescriptions via Surescripts more than doubled from 12.1 percent to 26 percent between 2008 and 2009, the year Medicare began paying bonuses to qualifying e-prescribing physicians under the Medicare Electronic Prescribing Incentive Program, established by the 2008 Medicare Improvements for Patients and Providers Act (MIPPA).14 The number of physician requests to Surescripts for patient medication histories and formulary information grew even more rapidly over the same period.
Continued growth in adoption is expected as physicians begin qualifying for substantially larger incentives starting in 2011 through the Medicare or Medicaid Electronic Health Records Incentive Programs (EHR Incentive Programs), established by the 2009 American Recovery and Reinvestment Act (ARRA). E-prescribing is one area in which physicians must demonstrate meaningful use of EHRs to receive payments.15 Physician use of specific e-prescribing features also is expected to continue accelerating as requirements for physician use and for related EHR certification—to ensure the systems meet technical standards—become more stringent over three stages.16
Under one of the five mandatory Stage 1 e-prescribing-related requirements, physicians must generate and transmit more than 40 percent of permissible prescriptions electronically to pharmacies. This threshold may increase over subsequent stages. The initial requirements for formulary information and medication history, while less direct, increase the likelihood that physicians will have access to and use these functions as well. Certified EHRs must have the capability to run drug formulary checks, although physicians are not required to enable the function in Stage 1. But, enabling the function is one option from a menu of 10 items of which the physician must choose five to implement in this initial stage.
There are no existing requirements specifically centered on generic prescribing or using third-party medication history. However, medication history could help support another optional item, medication reconciliation—defined under the EHR Incentive Programs as the process of identifying the most accurate list of all medications a patient is taking by comparing the medical record to an external list of medications obtained from a patient, hospital or other provider.17 Requirements related to formulary information and medication reconciliation also may become more rigorous in Stages 2 and 3.
![]() hile most physicians interviewed for this study stressed the importance of generating accurate and complete patient medication lists, respondents in only four of the 24 practices reported that physicians routinely augmented their practice’s prescribing records and patient reports with review of third-party medication history at the point of prescribing. In a third of the 24 practices, the e-prescribing system did not have a feature to access patient medication histories or users were unaware of it. Three practices chose not to implement the feature, and the remaining nine practices implemented the feature but physicians did not use it routinely because of challenges with data availability, perceived usefulness and system design.
hile most physicians interviewed for this study stressed the importance of generating accurate and complete patient medication lists, respondents in only four of the 24 practices reported that physicians routinely augmented their practice’s prescribing records and patient reports with review of third-party medication history at the point of prescribing. In a third of the 24 practices, the e-prescribing system did not have a feature to access patient medication histories or users were unaware of it. Three practices chose not to implement the feature, and the remaining nine practices implemented the feature but physicians did not use it routinely because of challenges with data availability, perceived usefulness and system design.
Data availability and usefulness. First, respondents reported that data were not consistently available for all insured patients. In some communities, users noted that some health insurers with substantial market share did not participate. For example, according to respondents in a Greenville practice, fewer than half of the insurance companies in the market were participating, while a Lansing respondent noted that a local health insurer that covered about 20 percent of the practice’s patients did not share data.
Among patients with available records, data may not be displayed for other technical reasons. For example, eligibility checks sometimes failed because of inconsistencies in patient identifying data between practice and health plan/PBM records. Overall, practice estimates of the percentage of insured patients with available medication histories varied considerably, from 20 to 100 percent, with estimates concentrated at 50 percent.
Second, even when medication history was available for a specific patient, practice respondents often reported that information was out-of-date or incomplete. As one physician said, “The confusion to some degree comes…because it’s brought into our system with a limited amount [of information]—it says the medication and prescribing doctor’s name and may or may not have data such as quantity, patient instructions, refills.... So, they take whatever data they have and push it forward to us, but there’s no effort to make it complete.” Also, because the data are from adjudicated claims, any prescriptions that patients pay for fully out of pocket, such as the $4 generics sold by many large big-box and chain pharmacies, are not included.
Finally, a patient’s medication history based on adjudicated claims is not equivalent to an active medication list. As an e-prescribing system vendor said, “There is no reconciliation before [the data] comes. The medication history…may have some drugs multiple times if there were multiple fills…[or] medications that the patient is no longer on.” As a result, as one prescriber explained, “It takes time to clean out the junk that ends up there in terms of duplications. It’s inconsistent as to whether everything a patient is taking is there [so] I can’t rely on what’s online for a complete list.”
Respondents in practices with access to the medication history function had mixed views about the value of the data. Practices that did not implement the feature cited problems getting access to useful data. In one of these practices, the physician respondent—a pediatric specialist—saw great potential in having access to this information for medication reconciliation. Nonetheless, according to the IT staff, “It’s not turned on. We receive many [data] errors when we attempt to test the functionality. We’re still working through some of those bugs.”
At the other extreme are the four practices that reported that physicians frequently used the feature in reviewing medication lists with patients. In one doctor’s view, “[quality of care is] light years ahead of where it was when we didn’t have the [patient medication history] information…Sometimes it might be incomplete for reasons we described, but I don’t know how to make the system any better.”
Several physicians who did not frequently use the feature found the data valuable for use on an ad hoc basis—for example, in cases of patients with complicated prescription use, to check the names of medications when patients cannot remember them, or to assist in identifying patient drug-seeking behavior. One physician explained: “I look at it [medication history]...if there’s a comprehensive visit, like a physical, or if I’m trying to manage a problem in a patient that’s seeing several other physicians….Or when they say ‘no, now I’m on the blue pill’….If you have a same-day patient…a sprained ankle…I don’t do the check for that.”
Other physicians did not believe there were compelling reasons to look at the medication history. One cardiologist echoed what some other physicians said when asked how often they looked at the data: “Rarely. Most patients we know well.” As the IT manager in that practice explained, “One problem is that the EMR is such a huge product and there’s so much going on with the patient that for the doctors to pull up one more thing, especially if it’s not utterly relevant or they don’t have a question, they won’t do it.”
System design. Design of the medication history tool, which varies substantially across e-prescribing systems, affected physician awareness of the feature, as well as their willingness to use it. Some systems displayed medication history prominently at the start of a prescribing session, along with patients’ active medications. In other cases, the user had to navigate from a prescription in progress to another window or screen to access this information. These “extra clicks” often dissuaded physicians from incorporating the step into their workflow. In addition, some practice respondents reported that medication histories were not available when renewing medications. Some e-prescribing vendors confirmed this was the case with their products as a result of their systems’ designs.
Data presentation also influenced physician use. One physician observed that few physicians in his practice used the medication history feature because the display was difficult to understand. “Horizontal lines show you the period for which the patient is presumed to have taken the medication… I like the idea of having that information, but you look at those horizontal lines and go ‘man, I can’t deal with this’ and then you go on,” he said. In another practice, the physician pointed out that the history was sorted by medication to help physicians de-duplicate the medication list more easily.
In addition to how and where the medication history data were displayed, e-prescribing systems varied in the ease with which physicians were able to act on the information, for example, to add a medication to a patient’s list or to prescribe it. In some systems, a single click was all that was required to copy the entry into the patient’s record. In other cases, the physician needed to take multiple steps to import the information, or, if the information was available as “view only,” the physician had to manually enter the information, which may have been on a different screen.
![]() ractices were more likely to have access to formulary data than medication history data, with respondents in almost all of the practices (22 of 24) reporting that this feature was available in their e-prescribing systems. Of the remaining two practices, one physician respondent became aware of the feature during the interview, and in the other practice, the e-prescribing vendor was implementing the feature. However, as with medication history, even when the feature was available, about half of the physicians reported that they and their colleagues reviewed the formulary data only occasionally, identifying similar challenges related to data availability and usefulness, as well as system design.
ractices were more likely to have access to formulary data than medication history data, with respondents in almost all of the practices (22 of 24) reporting that this feature was available in their e-prescribing systems. Of the remaining two practices, one physician respondent became aware of the feature during the interview, and in the other practice, the e-prescribing vendor was implementing the feature. However, as with medication history, even when the feature was available, about half of the physicians reported that they and their colleagues reviewed the formulary data only occasionally, identifying similar challenges related to data availability and usefulness, as well as system design.
Data availability and usefulness. As with medication history, respondents observed that formulary information was inconsistently available because health insurers may not have been participating or the patient matching process may have resulted in missing or incorrect data. Because formulary details were typically provided only for an insurer’s most popular products, respondents noted that data were sometimes inaccurate because a patient’s coverage differed from the typical product or was simply missing.
For example, at one Indianapolis practice, formulary information was unavailable for a large number of patients employed by an affiliated hospital system, even though it was available for other patients with coverage through the same insurer. Overall, respondents estimated that formulary data were available for anywhere from 20 percent to 100 percent of insured patients, with estimates clustered in the 50-80 percent range. Respondents in several practices noted that their physicians addressed such gaps by supplementing the data from their e-prescribing system with another electronic data source. “We all have quick access to Epocrates...If we have [a patient on] a smaller [insurer] we can quickly flip into that to see if we have some information,” a physician said.
Even when formulary data were available, some respondents perceived that the data were out of date or had limited usefulness. Respondents in some practices noted that formulary data were outdated, for example, because files were updated only sporadically given human resource or system hardware constraints, as practices may download numerous large files at once.18 One practice chose to delay implementing the formulary feature because of perceptions of low insurer participation and outdated information. As the IT manager said, “If you program the doctors that the [formulary] information won’t be there 80 percent of the time, it’s only a short amount of time before….they won’t use it because the click costs them time without information most of the time.”
Respondents in practices using the formulary feature reported that the most commonly displayed information was formulary status, followed by patient copayment tiers. While some physicians indicated that their system provided preferred formulary alternatives, others expressed preferences to see such information, as well as other, more-detailed information, such as a patient’s actual copayment amounts and whether a medication requires prior authorization.
The extent to which the data were valued and used by physicians also depended on individual prescribing preferences. A number of physicians indicated that they and their colleagues rarely used the feature because they nearly always prescribed generics or relied on pharmacists to make generic substitutions. Or, they mainly prescribed a small number of familiar medications, so they did not need supplementary data. As an example, one physician said, “I don’t know and never look for formulary information because I’m either prescribing a generic or prescribing a very specific medication for a specific problem.”
System design. As with medication history, system design varied across software vendors and influenced prescriber use. One physician said, “There are no real challenges to using formulary information. It is actually very simple to use. Under the formulary tab... [the medication list] is like a spreadsheet and the formulary shows yellow, green and red dots. It’s very clear.” Moreover, respondents in several practices noted that, in the systems they used, the formulary reminders were integrated into physicians’ workflow at multiple points, increasing the likelihood physicians would see and use the information: formulary status icons next to drug names in the initial medication search, suggested alternatives at initial drug selection, and a prompt before transmittal to the pharmacy, confirming if the physician wishes to send a non-formulary drug option.
In contrast, other users indicated that it was easy for physicians to overlook the feature, with one respondent explaining: “In the system you have an option to search for a drug using one button, the ‘prescribe new’ button, but if you do it that way you don’t get formulary information. There is another button that says ‘use formulary.’ I don’t know what percentage of time doctors use one button vs. another.” As with medication histories, formulary information was rarely displayed for renewals because of system design.
System design also affected how easy it was for physicians to change prescribing decisions based on formulary information. A physician in one practice found the formulary information easy to act on, saying, “On the list of medications I use commonly, the icons show up so I know before I select [the drug] if it’s on-formulary….if not, the easiest thing is to pull that medicine down, hit the alternatives button to find one [the insurance] will cover, and there’s a button that says ‘swap’ in that alternatives window and it just changes the prescription to the covered medicine.”
In another practice, the software provided formulary alternatives after the medication was selected, but the prescriber had to manually replace the existing selection rather than automatically importing the preferred drug. In yet another case, the system did not provide formulary alternatives at all. If the selected medication was off-formulary, the prescriber had to back out and make another selection. As the respondent described, “If you select Atacand [a blood pressure medicine]…and it comes up as non-formulary, the system does not spit out that this drug is not on formulary but these other three are. What I would have to do is enter another drug and hope that one is formulary…It’s a back-and-forth trial and error kind of thing.”
Overall, about two in five physician respondents believed that physicians in their practices were more likely to prescribe on-formulary or generic medications because of e-prescribing features. However, many of these physicians believed that the volume of formulary-related pharmacy callbacks was still burdensome, a perception held more generally across more than two-thirds of the practices.19 Respondents attributed this, at least in part, to the fact that many formulary-related calls were about obtaining prior authorizations, a process not supported by e-prescribing. As a result, practices continued to rely on pharmacies to alert them of the need for prior authorization after the e-prescription was sent, resulting in inefficiencies for both parties.
![]() o support generic prescribing, independent of whether formulary information was available or used, most practices noted that their e-prescribing systems defaulted to allow substitutions, so that even when a physician selected a brand-name medication, pharmacists were permitted to dispense a generic. Physicians wanting to guarantee that a brand-name drug was dispensed then had to manually override the default by selecting the instruction “dispense as written.”
o support generic prescribing, independent of whether formulary information was available or used, most practices noted that their e-prescribing systems defaulted to allow substitutions, so that even when a physician selected a brand-name medication, pharmacists were permitted to dispense a generic. Physicians wanting to guarantee that a brand-name drug was dispensed then had to manually override the default by selecting the instruction “dispense as written.”
While some practices reported relying primarily on pharmacies to make substitutions, others, desiring to actively select generic alternatives when writing prescriptions, described using additional e-prescribing tools to prompt physicians so they did not have to rely on recall. Two-thirds of practices had systems that displayed therapeutically equivalent generic alternatives based on information provided in medication databases sold by First Databank, Multum, Medi-Span or other companies to e-prescribing vendors.
Recognizing that physicians may be more likely to recall a brand name when searching for a medication, most of these systems reportedly returned both generic and brand-name equivalents regardless of which was queried. A few systems went further, substituting the generic name automatically unless the physician indicated that the prescription was to be dispensed as written. Some practices also mentioned proactively incorporating generic or chemical names into saved “favorites” lists so that physicians did not need to remember them.
![]() hysician access to e-prescribing systems with the features discussed in this study is likely to continue accelerating as more physicians adopt e-prescribing, more e-prescribing vendors offer products with these features and physicians already e-prescribing upgrade to newer versions certified under the EHR Incentive Programs.20
hysician access to e-prescribing systems with the features discussed in this study is likely to continue accelerating as more physicians adopt e-prescribing, more e-prescribing vendors offer products with these features and physicians already e-prescribing upgrade to newer versions certified under the EHR Incentive Programs.20
Current and proposed federal requirements related to formulary and medication history do not, however, directly require physicians to review the information when making prescribing decisions. Consistent with earlier research, this study’s findings suggest that barriers still impede physicians’ use of these data in making prescribing decisions. Physicians in this study who saw a need for the data, who perceived that the data were sufficiently complete and accurate, and who used e-prescribing systems that facilitated viewing and acting on the information were more likely to use the features.
To the extent that policy makers and other stakeholders want to promote greater prescriber use of medication histories and patient formulary information, the following activities have potential to enhance the value of the data and reduce the time costs of accessing and acting on it:
Increasing data availability and usefulness. Encouraging increased health insurer and Medicaid program participation and the provision of more accurate and complete medication history and formulary information—as already required by health insurers and PBMs participating in the Medicare Part D program—could enhance the value of e-prescribing to physicians. In addition, making pharmacy fill data, which Surescripts currently collects, consistently available to e-prescribing systems would provide physicians with information on medications paid out of pocket by both insured and uninsured patients. More comprehensive medication histories may increase the value to physicians of using this feature when selecting medications and for medication reconciliation more generally. More comprehensive medication histories also may support improved drug interaction alerts. However, including additional information sources could compound the challenge of reconciling different lists, for example, by increasing the number of duplicate medications.
Some joint federal-industry efforts underway to develop additional e-prescribing technical standards might help address this challenge and enhance the value of the data in other ways. According to experts, the implementation of RxNorm, a technical standard for medication names, potentially may enhance e-prescribing vendors’ ability to reconcile medication histories from multiple sources using different naming conventions.21 In addition, standardizing drug names could support the more frequent return of accurate formulary information and make it easier to provide more comprehensive formulary and benefit information reflecting a patient’s specific coverage.22 While use of RxNorm is not currently required as part of the EHR certification in Stage 1 of the EHR Incentive Programs, the federal government expressed interest in doing so in later stages.23
Technical standards to support real-time access to up-to-date formulary information, for example, similar to the information PBMs currently provide to pharmacies, and to support prior authorizations also have been explored.24 If successfully implemented, use of these standards also might substantially enhance the value of the formulary feature to physician practices and improve both physician practice and pharmacy efficiency.
Enhancing system design. E-prescribing systems with easier-to-use designs may increase physician awareness of features at adoption and as updated versions with enhanced features are implemented. Vendors likely will more proactively enhance system design and features related to specific requirements of the EHR Incentive Programs. For example, one e-prescribing vendor respondent noted that the firm would soon be introducing the ability to import items from the medication history screen in response to requirements related to medication reconciliation—a feature many physicians noted was lacking in their e-prescribing systems.
Nonetheless, more systematic usability studies and development of best practices across vendors could be valuable in promoting more uniform improvements in system design and potentially help guide physicians in purchasing systems that better meet their needs.25
Targeted physician education and training. While enhanced system design may help make features more attractive to physicians, targeted education and training likely will continue to be necessary, particularly for physicians faced with using EHRs to support a broad range of clinical activities to qualify for incentive payments. The study findings suggest that physicians and other practice staff could benefit from more education or training on specific functionalities, especially after they have started using the system and are competent with the basic functionality.
While such efforts are supported by IT staff in larger physician practices, e-prescribing vendors, Surescripts and other stakeholders, challenges to training will grow as users are confronted with implementing the full range of requirements under the EHR Incentive Programs. The Health Information Technology Regional Extension Centers and the related Health Information Technology Research Center were created under ARRA to assist primary care clinicians in smaller practices, among other providers, in adopting EHRs and qualifying for incentive payments. These organizations may help overcome barriers to implementation of e-prescribing features and work with the various parties to enhance data value, system design and approaches to effective physician education and training.
The federal incentive programs likely will provide a strong catalyst for moving toward more robust and effective use of e-prescribing. This study’s finding that physician perceptions of the value of data for patient care must outweigh time costs of using the information suggests, however, that additional efforts likely will be required by many stakeholders to meet policy makers’ ultimate goals of encouraging physicians to become meaningful users of EHRs.
| 1. | eHealth Initiative, Electronic Prescribing: Becoming Mainstream Practice (June 2008); Surescripts, Advancing Healthcare In America: 2009 National Progress Report On E-Prescribing (2010); U.S. Department of Health and Human Services (HHS), Office of Inspector General (OIG), Medicare Part D Plan Sponsor Electronic Prescribing Initiatives, Memorandum No. OEI-05-08-00322, Washington, D.C. (October 2009). |
| 2. | Surescripts provides pharmacy fill data, which includes cash sales to both insured and uninsured patients, to health information exchanges and other organizations. However, at the time of the study, these data were not widely available to e-prescribers. |
| 3. | Bell, Douglas S., et al., “Evaluating the Technical Adequacy of Electronic Prescribing Standards: Results of an Expert Panel Process,” AMIA Annual Symposium Proceedings (2008). |
| 4. | Bell (2008). |
| 5. | HHS, OIG, Medicare Part D E-Prescribing Standards: Early Assessment Shows Partial Connectivity, Report No. OEI-05-08-00320, Washington, D.C. (October 2009). |
| 6. | Surescripts (2010). |
| 7. | Surescripts, 2009 State Progress Reports on E-Prescribing, available at http://www.surescripts.com/about-e-prescribing/progress-reports/state-progress-reports.aspx. (Accessed May 2, 2011.) |
| 8. | See, for example, Fischer, Michael A., et al., “Effect of Electronic Prescribing with Formulary Decision Support on Medication Use and Cost,” Archives of Internal Medicine, Vol. 168, No. 22 (December 2008); Stenner, Shane P., et al., “Impact of Generic Substitution Decision Support on Electronic Prescribing Behavior,” Journal of the American Medical Informatics Association, Vol. 17, No. 6 (November 2010); Wang, C. Jason, et al., “Perceptions of Standards-Based Electronic Prescribing Systems as Implemented in Outpatient Primary Care: A Physician Survey,” Journal of the American Medical Informatics Association, Vol.16, No. 4 (July/August 2009). |
| 9. | Simonaitis, Linas, Anne Belsito and J. Marc Overhage, “Enhancing an ePrescribing System by Adding Medication Histories and Formularies: the Regenstrief Medication Hub,” AMIA Annual Symposium Proceedings (2008); Grossman, Joy M., Even When Physicians Adopt E-Prescribing, Use Of Advanced Features Lags, Issue Brief No. 133, Center for Studying Health System Change, Washington D.C. (July 2010); Surescripts (2010). |
| 10. | DesRoches, Catherine M., et al., “Differences between Integrated and Stand-Alone E-Prescribing Systems Have Implications for Future Use,” Health Affairs, Vol. 29, No.12 (December 2010). |
| 11. | Grossman, Joy M., et al., “Physicians’ Experiences Using Commercial E-prescribing Systems,” Health Affairs, Web exclusive (April 3, 2007); National Opinion Research Center at the University of Chicago, Findings from the Evaluation of E-Prescribing Pilot Sites, AHRQ Publication No. 07-0047-EF, Rockville, Md. (April 2007); Bell (2008); Wang (2009). See also more recent expert perspectives, for example, Overhage, J. Marc, “Testimony to the HIT Policy Committee Information Exchange Group on ePrescribing and Meaningful Use” (Jan. 25, 2010) and Center for Improving Medication Management, The Road to Meaningful Use: Leveraging E-Prescribing to Improve Medication Management, Collaborative Forum Summarized Content, Chicago (April 29, 2010). |
| 12. | Respondents were asked whether their practice’s e-prescribing system was a stand-alone system or part of an electronic medical record (EMR) system. EMRs also are frequently referred to as EHRs, the term used in this Research Brief. The ratio of EHRs to stand-alone systems used by the practices in this study is closely representative of the distribution among physicians registered nationally on Surescripts in 2009 (Surescripts (2010)). |
| 13. | U.S. Government Accountability Office, Electronic Prescribing: CMS Should Address Inconsistencies in Its Two Incentive Programs That Encourage the Use of Health Information Technology, Publication No. GAO-11-159, Washington, D.C. (Feb. 17, 2011). |
| 14. | Surescripts (2010). |
| 15. | For a detailed comparison of the MIPPA and ARRA e-prescribing programs, see GAO (2011). |
| 16. | See, for example, HHS Office of the National Coordinator for Health Information Technology, Health IT Policy Committee, Meaningful Use Workgroup Request for Comments Regarding Meaningful Use Stage 2, Washington, D.C. (January 2011), available at http://healthit.hhs.gov/media/faca/MU_RFC_2011-01-12_final.pdf. |
| 17. | Centers for Medicare and Medicaid Services, Eligible Professional Meaningful Use Menu Set Measures, Measure 7 of 10: Medication Reconciliation, EHR Incentive Programs, Baltimore (November 2010). |
| 18. | Overhage (2010). |
| 19. | This finding is consistent with other studies. See, for example, Wang (2009). |
| 20. | The number of vendors that Surescripts has certified for medication history and formulary and benefit services recently has increased rapidly, likely at least in part in response to the federal incentive program under MIPPA. See Surescripts (2010). |
| 21. | Bell (2008); Bell, Douglas S., et al., Evaluation of RxNorm in Ambulatory Electronic Prescribing, RAND Technical Report No. TR-941-CMS, Santa Monica, Calif. (In Press 2011). |
| 22. | Bell (2008); Bell (In Press 2011). |
| 23. | HHS, Office of the Secretary, 45 CFR Part 170 Health Information Technology: Initial Set of Standards, Implementation Specifications, and Certification Criteria for Electronic Health Record Technology, Interim Final Rule (Jan. 13, 2010). |
| 24. | HHS, OIG, Report No. OEI-05-08-00320 (October 2009); Bell, Douglas S., et al., Pilot Testing of Electronic Prescribing Standards, AHRQ (April 2007). |
| 25. | See, for example, Armijo Dan, Cheryl McDonnell, and Kristen Werner, Electronic Health Record Usability: Interface Design Considerations, AHRQ Publication No. 09(10)-0091-2-EF (2009) and RAND, A Toolset for E-Prescribing Implementation, Santa Monica, Calif. (forthcoming). |
This study is part of a larger qualitative research project on physician practice and pharmacy experiences with e-prescribing, which included 114 telephone interviews conducted between February and September 2010. Respondents were interviewed in 24 physician practices and 48 community pharmacies actively transmitting prescriptions electronically via Surescripts, the largest prescription transmission network in the United States. Sampling frames were developed from lists available on the company’s Web site of Surescripts-registered physicians and pharmacies located in 12 Community Tracking Study sites—Boston; Cleveland; Greenville, S.C.; Indianapolis; Lansing, Mich.; Little Rock, Ark.; Miami; northern New Jersey; Orange County, Calif.; Phoenix; Seattle; and Syracuse, N.Y. Two physician practices and four pharmacies in each of the 12 communities participated. In each practice, one physician user was interviewed who provided a clinical perspective on the experiences of prescribers in the practice, and a second interview was conducted in 15 practices that had people responsible for managing the e-prescribing system—typically an IT manager or a nurse—if they were better able to provide a technical and operational perspective. In each pharmacy, the pharmacist-in-charge was interviewed. Additional respondents included national representatives of mail-order pharmacies, chain pharmacies, e-prescribing and pharmacy system vendors, e-prescribing intermediaries, and medication database vendors. Interviews were conducted by two-person research teams using semi-structured protocols. Notes were transcribed and jointly reviewed for quality and validation purposes. The interview responses were coded and analyzed using Atlas.ti, a qualitative software tool.
This research was funded by the Agency for Healthcare Research and Quality (AHRQ) under Contract No. 290-05-0007 (03). The views expressed are the authors’ and do not necessarily represent the position of AHRQ or the U.S. Department of Health and Human Services. .
RESEARCH BRIEFS are published by the Center for Studying Health System
Change.
600 Maryland Avenue, SW, Suite 550
Washington, DC 20024-2512
Tel: (202) 484-5261
Fax: (202) 484-9258
www.hschange.org