Data Bulletin No. 36
December 2010
James D. Reschovsky, Alwyn Cassil, Hoangmai H. Pham
![]() olicy makers have long been concerned that physicians with ownership or other financial interests in medical facilities and equipment would make more referrals than medically necessary. And, a substantial body of research indicates that physician ownership of facilities and equipment does affect referral patterns.1
olicy makers have long been concerned that physicians with ownership or other financial interests in medical facilities and equipment would make more referrals than medically necessary. And, a substantial body of research indicates that physician ownership of facilities and equipment does affect referral patterns.1
In 1989, Congress enacted the federal physician self-referral law, commonly known as the Stark Act after U.S. Rep. Pete Stark of California. The law took effect in 1992 and barred physician self-referrals of Medicare patients for clinical laboratory services. Later, the Stark law was expanded to cover Medicaid patients and other health services, including inpatient and outpatient hospital services and radiology services. However, there are numerous exceptions to the self-referral prohibitions, most notably if the service is provided within the physician’s office or practice.
Since the enactment of the Stark laws, technological advances have allowed more services to be provided in outpatient settings, including physicians’ offices. At the same time, the cost and scale of high-tech equipment, including advanced imaging equipment, such as computed tomography (CT) and magnetic resonance imaging (MRI) scanners, has declined, making office-based installations more feasible from a business perspective.
While previous research on physician self-referral has focused on particular services, such as advanced imaging, there has been little national information about how pervasive physician ownership or leasing of medical equipment is more broadly. HSC’s nationally representative 2008 Health Tracking Physician Survey asked physicians whether their main practice owned or leased equipment used for:
Of the 2,750 physicians in community-based, physician-owned practices—who represent 58 percent of all physicians—25.2 percent reported their practice owned/leased equipment for laboratory services, 22.7 percent for X-rays, 17.4 percent for advanced imaging, 28.9 percent for non-invasive procedures and 11.4 percent for invasive procedures (see Table 1). Overall, almost one in seven physicians (13.2%) reported that their practice owned or leased three or more types of equipment.
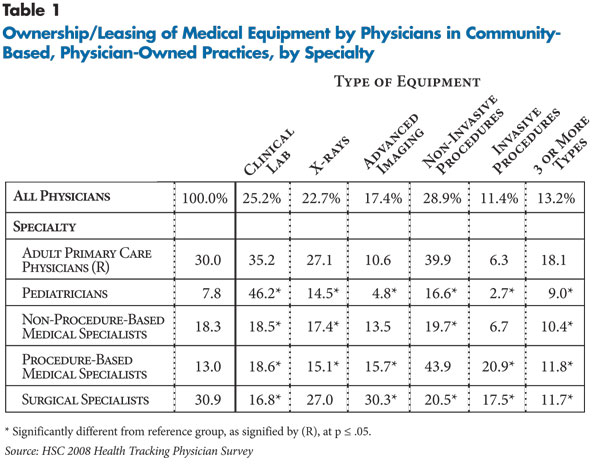
![]() cross the various equipment categories, rates of ownership varied significantly by physician specialty. Primary care physicians treating adults were more likely than other physicians except pediatricians to own laboratory testing equipment, while primary care physicians treating adults and surgeons were more likely to own X-ray equipment.
cross the various equipment categories, rates of ownership varied significantly by physician specialty. Primary care physicians treating adults were more likely than other physicians except pediatricians to own laboratory testing equipment, while primary care physicians treating adults and surgeons were more likely to own X-ray equipment.
Although surgeons were more likely to own equipment for advanced imaging (30.3%), 10.6 percent of primary care physicians treating adults; 13.5 percent of non-procedure-based medical specialists,2 such as neurologists; and 15.7 percent of procedure-based medical specialists, such as cardiologists, also owned advanced imaging equipment.
About one in four primary care physicians treating adults and procedure-based specialists owned equipment for non-invasive procedures, and 20.9 percent of procedure-based specialists and 17.5 percent of surgeons owned equipment for invasive procedures.
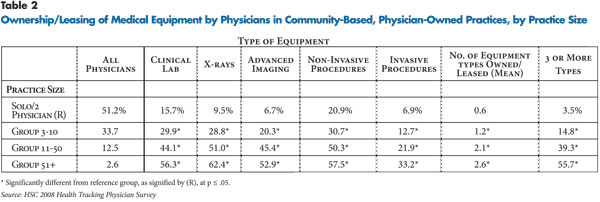
![]() onsistently, equipment ownership was more likely the larger the practice, where the equipment can be used more consistently and costs recouped more quickly. A majority of physicians in the largest practices—more than 50 physicians—owned equipment for laboratory services, X-rays, advanced imaging and non-invasive procedures (see Table 2).
onsistently, equipment ownership was more likely the larger the practice, where the equipment can be used more consistently and costs recouped more quickly. A majority of physicians in the largest practices—more than 50 physicians—owned equipment for laboratory services, X-rays, advanced imaging and non-invasive procedures (see Table 2).
However, about two in 10 physicians in the smallest practices—solo or two physician—owned equipment for non-invasive procedures and 15.7 percent owned equipment for laboratory testing. And, slightly less than a third of physicians practicing in groups of three to 10 physicians owned laboratory, X-ray and non-invasive procedure equipment, while 20.3 percent owned advanced imaging equipment.
![]() esponding to rapid increases in Medicare spending on advanced imaging services, Congress and the Centers for Medicare and Medicaid Services have acted in recent years to make physician ownership and use of some types of advanced imaging less attractive by cutting Medicare reimbursements. Additionally, under the health reform law, starting Jan. 1, 2011, physicians who refer Medicare and Medicaid patients for certain advanced imaging services, including MRI and CT scans, within their practices must disclose their financial interest and provide patients with a list of alternative suppliers.3
esponding to rapid increases in Medicare spending on advanced imaging services, Congress and the Centers for Medicare and Medicaid Services have acted in recent years to make physician ownership and use of some types of advanced imaging less attractive by cutting Medicare reimbursements. Additionally, under the health reform law, starting Jan. 1, 2011, physicians who refer Medicare and Medicaid patients for certain advanced imaging services, including MRI and CT scans, within their practices must disclose their financial interest and provide patients with a list of alternative suppliers.3
Given the growing evidence that physician self-referral contributes to unnecessary and costly care,4 policy makers might reconsider the broadness of the in-office ancillary service exemption to the Stark law. Ultimately, moving away from fee-for-service payment toward payment mechanisms that reimburse physicians for a broader unit of service, such as an episode of care, or putting physicians at least partially at risk for the cost of care will alter the financial incentives that now encourage physician self-referrals.
| 1. | See for example, Casalino, Larry P., Physician self-referral and physician-owned specialty facilities, Research Synthesis Report No. 15., Robert Wood Johnson Foundation, Princeton, N.J. (June 2008); and Mitchell, Jean M., The Prevalence of Physician Self-referral Arrangements after Stark II: Evidence from Advanced Diagnostic Imaging, Health Affairs, Vol. 26, No. 3 (May/June 2007). |
| 2. | The HSC 2008 Health Tracking Physician Survey identifies physicians by the following three broad specialty categories: primary care, medical specialist and surgical specialist. Medical specialists have been further classified as non-procedure-base medical specialists and procedure-based medical specialists. See www.hschange.org/CONTENT/1172/HSCPhysicianList.pdf or a full description of the specialty classifications. |
| 3. | Patient Protection and Affordable Care Act (Public Law No. 111-148), Section 6003. |
| 4. | Health Affairs, “Health Affairs Studies Puncture Arguments About Benefits of Physicians’ Self-Referrals for Imaging,” News Release (Dec. 8 2010). |
This Data Bulletin presents findings from the Center for Studying Health System Change (HSC) 2008 Health Tracking Physician Survey, a nationally representative mail survey of U.S. physicians providing at least 20 hours per week of direct patient care. The sample of physicians was drawn from the American Medical Association master file and included active, nonfederal, office- and hospital-based physicians. Residents and fellows were excluded, as well as radiologists, anesthesiologists and pathologists. The survey includes responses from more than 4,700 physicians, and the response rate was 62 percent. Since this Data Bulletin examines the extent of physician practice ownership or leasing of medical equipment, the sample was limited to 2,750 physicians practicing in community-based, physician-owned practices. Physicians employed by hospitals, who practiced in hospital-based settings or who worked in hospital-owned practices were excluded. More detailed information on survey content and methodology can be found at www.hschange.org.
This research was supported by the Robert Wood Johnson Foundation.
RESEARCH BRIEFS are published by the Center for Studying Health System
Change.
600 Maryland Avenue, SW, Suite 550
Washington, DC 20024-2512
Tel: (202) 484-5261
Fax: (202) 484-9258
www.hschange.org