
Issue Brief No. 129
December 2009
Emily Carrier, James D. Reschovsky
Use of care management tools—such as group visits or patient registries—varies widely among primary care physicians whose practices care for patients with four common chronic conditions—asthma, diabetes, congestive heart failure and depression—according to a new national study by the Center for Studying Health System Change (HSC). For example, less than a third of these primary care physicians in 2008 reported their practices use nurse managers to coordinate care, and only four in 10 were in practices using registries to keep track of patients with chronic conditions. Physicians also used care management tools for patients with some chronic conditions but not others. Practice size and setting were strongly related to the likelihood that physicians used care management tools, with solo and smaller group practices least likely to use care management tools. The findings suggest that, along with experimenting with financial incentives for primary care physicians to adopt care management tools, policy makers might consider developing community-level care management resources, such as nurse managers, that could be shared among smaller physician practices.
![]() mproving the care of patients with chronic conditions is
a priority for policy makers as both the prevalence and costs of chronic disease
in the United States increase. By one estimate, the care of chronic conditions
accounts for about 75 percent of U.S. health care spending, or about $1.5 trillion,
annually.1 Previous research has shown that care management
tools, ranging from nurse managers to patient registries to identify patients
with chronic conditions, can improve care processes and outcomes for patients
with chronic conditions.
mproving the care of patients with chronic conditions is
a priority for policy makers as both the prevalence and costs of chronic disease
in the United States increase. By one estimate, the care of chronic conditions
accounts for about 75 percent of U.S. health care spending, or about $1.5 trillion,
annually.1 Previous research has shown that care management
tools, ranging from nurse managers to patient registries to identify patients
with chronic conditions, can improve care processes and outcomes for patients
with chronic conditions.
However, some care management tools work better than others. Interventions using team-based care—such as nurse managers and nonphysician patient educators—as well as group visits have been associated with better control of diabetes and other chronic conditions, while provision of written patient education materials is less effective.2 Likewise, research has shown that automated reminder systems and prompts to perform certain care are more effective than other alternatives offering less-specific and less-timely feedback to individual physicians.3
Among primary care physicians caring for adult patients in 2008, 91 percent were in practices treating patients with four common chronic conditions—asthma, diabetes, congestive heart failure and depression, according to findings from HSC’s nationally representative 2008 Health Tracking Physician Survey (see Data Source). Yet, these physicians’ use of care management tools varied widely, and interventions backed by the strongest evidence of effectiveness were used much less frequently. Both practice size and setting, as well as the specific chronic condition being treated, were strongly associated with the use of certain care management tools.
The survey asked physicians whether their practices used:
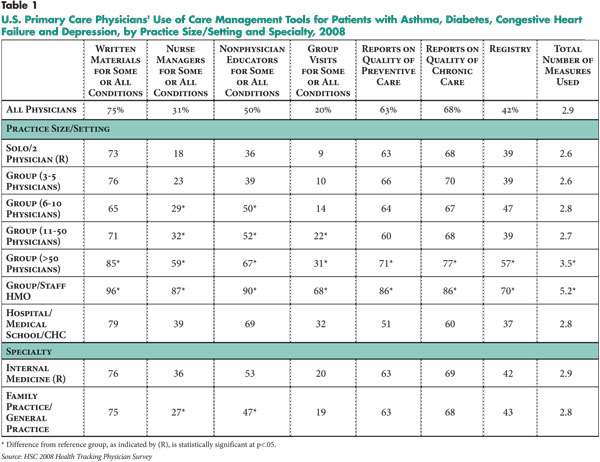
Three-quarters of physicians reported offering patients written educational materials, but use of other tools for patient education and improved self-care was much lower (see Table 1). Half of physicians reported using nonphysician educators, one-third used nurse managers and one-fifth used group visits. The higher use of written patient education materials may reflect expediency rather than effectiveness. Written materials are inexpensive and require little upfront investment compared with the other interventions described, but they are also associated with the least benefit.4
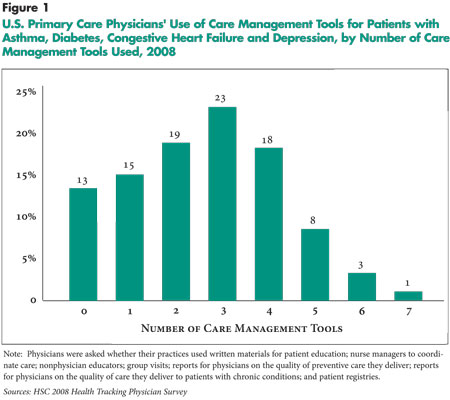
Physicians more uniformly used tools offering feedback on the quality of their care, which can help identify areas for improvement. About two-thirds of physicians reported receiving reports on the quality of their preventive and chronic care, and 42 percent used registries to identify patients with specific chronic conditions. However, some of these reports and registries may be generated by patients’ insurers rather than by physician practices and thus may not apply to all patients treated by a practice. Overall, 47 percent of physicians were in practices that used two or fewer of the seven care management tools, and 4 percent were in practices using six or seven care management tools (see Figure 1).
![]() hysicians’ adoption of care management tools varied significantly by how their practices were organized. Physicians in larger groups were more likely to use nearly every type of care management tool than physicians in solo or two-physician practices. Likewise, physicians in group- or staff-model health maintenance organizations (HMOs) were the most likely to use all of the care management tools.
hysicians’ adoption of care management tools varied significantly by how their practices were organized. Physicians in larger groups were more likely to use nearly every type of care management tool than physicians in solo or two-physician practices. Likewise, physicians in group- or staff-model health maintenance organizations (HMOs) were the most likely to use all of the care management tools.
For example, about one in 10 physicians in solo or two-physician practices reported using group visits, compared with about three in 10 physicians in group practices of 50 or more physicians, and about seven in 10 physicians in group/staff HMOs. Similarly, about four in 10 physicians in solo or two-physician practices reported using patient registries, compared with almost six in 10 physicians in group practices of 50 or more physicians and seven in 10 physicians in group/staff HMOs.
Use of reports on the quality of preventive and chronic care varied less across practice settings. Eighty-six percent of physicians in group/staff HMOs received both types of feedback reports, compared with physicians in solo or two-physician practices where 63 percent received reports on preventive care and 68 percent received reports on chronic care.
Previous research also has found modest uptake of care management tools, but the studies have been limited to larger physician practices and do not reflect the experiences of the nearly two-thirds of physicians who work in practices with fewer than 20 physicians. In the 2008 Health Tracking Physician Survey, 14 percent of physicians were in practices of 20 physicians or more and reported similar rates of care management tool adoption on average as respondents in a 2006 national survey of similar-sized practices.5 The findings from the 2008 Health Tracking Physician Survey suggest that physicians practicing in smaller groups, whose uptake of care management tools had not previously been measured, are much farther behind.
Surprisingly, physicians who reported that most or all patients in their practice had chronic conditions were no more likely to use care management tools than physicians who reported few or no chronically ill patients. Among primary care physicians, there was little difference between general internists and family practitioners. By comparison, specialists—cardiologists, endocrinologists, pulmonologists and psychiatrists who treat patients with congestive heart failure, diabetes, asthma and depression, respectively—generally reported similar or lower rates of care management tool use as primary care physicians. One exception was endocrinologists, who were much more likely to report using nonphysician educators and group visits in the management of diabetes (findings not shown).
![]() mong primary care physicians whose practices treated patients
with asthma, diabetes, depression and congestive heart failure, most used care
management tools for patients with some conditions but not others (see Table
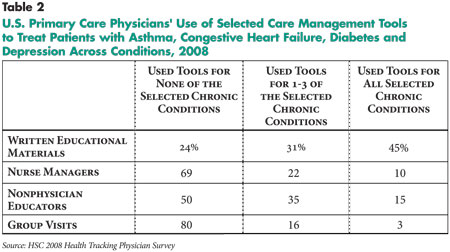
2). Physicians using tools in their practices for patient education and
improved self-care—written materials, nurse managers, nonphysician educators
and group visits—were asked about which tools they used for which conditions.
With the exception of written educational materials, less than 15 percent of
physicians reported using any tool across all four of the chronic conditions.
Care management tools aimed at patient education and improved self-care were
more widely adopted for diabetic and asthmatic patients.
mong primary care physicians whose practices treated patients
with asthma, diabetes, depression and congestive heart failure, most used care
management tools for patients with some conditions but not others (see Table
2). Physicians using tools in their practices for patient education and
improved self-care—written materials, nurse managers, nonphysician educators
and group visits—were asked about which tools they used for which conditions.
With the exception of written educational materials, less than 15 percent of
physicians reported using any tool across all four of the chronic conditions.
Care management tools aimed at patient education and improved self-care were
more widely adopted for diabetic and asthmatic patients.
![]() ealth information technology, particularly fully electronic medical record (EMR) systems, should provide physicians with easier ways to manage patients with chronic conditions. Typically, EMRs have features to generate reminders for physicians to provide preventive care and to generate patient reminders for preventive care.
ealth information technology, particularly fully electronic medical record (EMR) systems, should provide physicians with easier ways to manage patients with chronic conditions. Typically, EMRs have features to generate reminders for physicians to provide preventive care and to generate patient reminders for preventive care.
Less than one-third (29%) of primary care physicians reported having a fully electronic medical record. Among these physicians, slightly more than half (54%) used physician reminders to provide preventive care and one-third (34%) generated patient reminders.
![]() espite growing policy attention to improving care for people with chronic conditions, use of care management tools varies widely among primary care physicians. There are few financial incentives for physicians to bear the cost of adopting care management tools, particularly in a predominantly fee-for-service payment environment. Insurers will rarely reimburse physicians for resource-intensive types of care management, such as hiring nurse managers to coordinate care or additional staff to maintain patient registries.
Both public and private payers are experimenting with new payment approaches that would reward physicians that offer these and other services. In the medical-home model, for example, primary care practices can qualify for additional per-patient, per-month payments by demonstrating that they provide services aimed at organizing and coordinating care.
espite growing policy attention to improving care for people with chronic conditions, use of care management tools varies widely among primary care physicians. There are few financial incentives for physicians to bear the cost of adopting care management tools, particularly in a predominantly fee-for-service payment environment. Insurers will rarely reimburse physicians for resource-intensive types of care management, such as hiring nurse managers to coordinate care or additional staff to maintain patient registries.
Both public and private payers are experimenting with new payment approaches that would reward physicians that offer these and other services. In the medical-home model, for example, primary care practices can qualify for additional per-patient, per-month payments by demonstrating that they provide services aimed at organizing and coordinating care.
However, even with additional payments, it may not make sense for individual physician practices, particularly small practices, to invest in and develop the infrastructure for improved care management. Some care management tools are expensive to implement and only make financial sense in larger practices where economies of scale exist. Offering individual practices modest per-patient incentives to adopt care management tools does not address the problem that many of these practices are simply too small to support additional staff or other resources on an ongoing basis. Moreover, no single payer may represent enough of a physician’s patient panel to drive spending decisions.
An alternative approach would provide incentives for practices to join together in affiliated networks large enough to sustain a variety of practice innovations on their own.6 For example, Community Care of North Carolina, an offshoot of the state’s Medicaid program, has successfully created community-level resources and funded case managers that are shared among several small practices.
Networking and community-based resources may not be a panacea; even large practices that were not part of HMOs on average only used half of the care management tools studied. To strengthen the use of care management tools in primary care, physicians may require education and technical assistance above and beyond the incentives currently proposed.
This Issue Brief presents findings from the HSC 2008 Health Tracking Physician Survey, a nationally representative mail survey of U.S. physicians providing at least 20 hours per week of direct patient care. The sample of physicians was drawn from the American Medical Association master file and included active, nonfederal, office- and hospital-based physicians. Residents and fellows were excluded, as well as radiologists, anesthesiologists and pathologists. The survey includes responses from more than 4,700 physicians, and the response rate was 62 percent. The survey includes a subsample of 1,304 physicians who reported training in internal medicine or family practice, providing primary care for adults, and that their practice treats patients with diabetes, congestive heart failure, asthma and depression. Estimates from this survey should not be compared to estimates from HSC’s previous Community Tracking Study Physician Surveys because of changes in the survey administration mode from telephone to mail, question wording, skip patterns, sample structure and population represented. More detailed information on survey content and methodology can be found at www.hschange.org.
This research was funded by the Robert Wood Johnson Foundation.
RESEARCH BRIEFS are published by the Center for Studying Health System
Change.
600 Maryland Avenue, SW, Suite 550
Washington, DC 20024-2512
Tel: (202) 484-5261
Fax: (202) 484-9258
www.hschange.org